Chen Lu, Chen Guang-Qiang, Shore Kevin, Shklar Orest, Martins Concetta, Devenyi Brian, Lindsay Paul, McPhail Heather, Lanys Ashley, Soliman Ibrahim, Tuma Mazin, Kim Michael, Porretta Kerri, Greco Pamela, Every Hilary, Hayes Chris, Baker Andrew, Friedrich Jan O, Brochard Laurent
Interdepartmental Division of Critical Care Medicine, University of Toronto, Toronto, ON, Canada.
Keenan Research Centre and Li Ka Shing Institute, Department of Critical Care, St. Michael's Hospital, 209 Victoria Street, Room 408, Toronto, ON, M5B 1T8, Canada.
Crit Care. 2017 Apr 4;21(1):84. doi: 10.1186/s13054-017-1671-8.
Despite their potential interest for clinical management, measurements of respiratory mechanics in patients with acute respiratory distress syndrome (ARDS) are seldom performed in routine practice. We introduced a systematic assessment of respiratory mechanics in our clinical practice. After the first year of clinical use, we retrospectively assessed whether these measurements had any influence on clinical management and physiological parameters associated with clinical outcomes by comparing their value before and after performing the test.
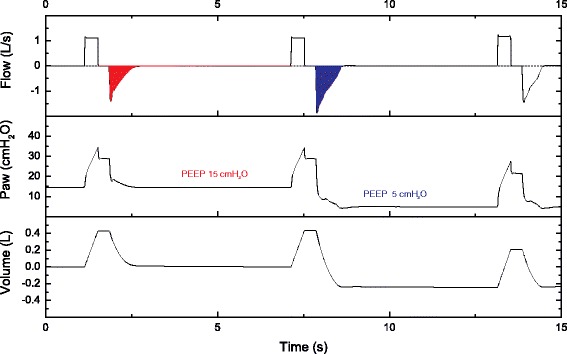
The respiratory mechanics assessment constituted a set of bedside measurements to determine passive lung and chest wall mechanics, response to positive end-expiratory pressure, and alveolar derecruitment. It was obtained early after ARDS diagnosis. The results were provided to the clinical team to be used at their own discretion. We compared ventilator settings and physiological variables before and after the test. The physiological endpoints were oxygenation index, dead space, and plateau and driving pressures.
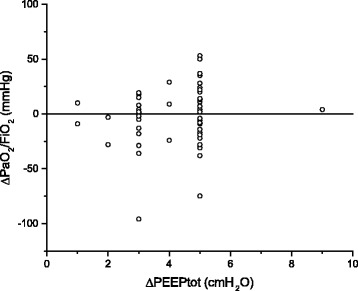
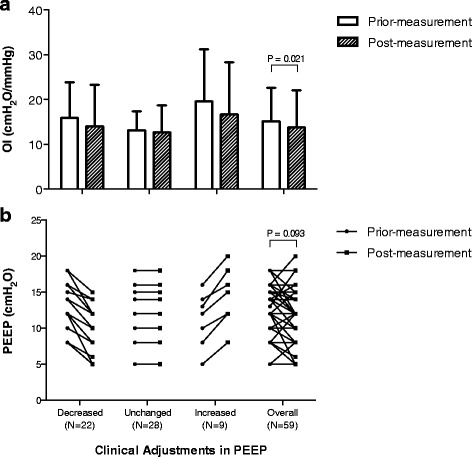
Sixty-one consecutive patients with ARDS were enrolled. Esophageal pressure was measured in 53 patients (86.9%). In 41 patients (67.2%), ventilator settings were changed after the measurements, often by reducing positive end-expiratory pressure or by switching pressure-targeted mode to volume-targeted mode. Following changes, the oxygenation index, airway plateau, and driving pressures were significantly improved, whereas the dead-space fraction remained unchanged. The oxygenation index continued to improve in the next 48 h.
Implementing a systematic respiratory mechanics test leads to frequent individual adaptations of ventilator settings and allows improvement in oxygenation indexes and reduction of the risk of overdistention at the same time.
The present study involves data from our ongoing registry for respiratory mechanics (ClinicalTrials.gov identifier: NCT02623192 . Registered 30 July 2015).
尽管呼吸力学测量对临床管理具有潜在意义,但在急性呼吸窘迫综合征(ARDS)患者中,常规临床实践中很少进行此类测量。我们在临床实践中引入了对呼吸力学的系统评估。在临床使用的第一年之后,我们通过比较测试前后的数值,回顾性评估这些测量是否对临床管理以及与临床结局相关的生理参数有任何影响。
呼吸力学评估包括一系列床旁测量,以确定被动肺和胸壁力学、对呼气末正压的反应以及肺泡去募集情况。在ARDS诊断后早期进行该评估。结果提供给临床团队,由他们自行决定是否使用。我们比较了测试前后的呼吸机设置和生理变量。生理终点指标为氧合指数、死腔、平台压和驱动压。
连续纳入61例ARDS患者。53例患者(86.9%)测量了食管压力。41例患者(67.2%)在测量后更改了呼吸机设置,通常是通过降低呼气末正压或从压力控制模式切换为容量控制模式。更改后,氧合指数、气道平台压和驱动压显著改善,而死腔分数保持不变。在接下来的48小时内氧合指数持续改善。
实施系统的呼吸力学测试可导致呼吸机设置频繁进行个体化调整,并同时改善氧合指数以及降低肺过度扩张风险。
本研究涉及我们正在进行的呼吸力学注册研究的数据(ClinicalTrials.gov标识符:NCT02623192。于2015年7月30日注册)。