Jabo Brice, Morgan John W, Martinez Maria Elena, Ghamsary Mark, Wieduwilt Matthew J
Loma Linda University School of Public Health, Loma Linda, California, United States of America.
University of California San Diego, Moores Cancer Center, La Jolla, California, United States of America.
PLoS One. 2017 Apr 6;12(4):e0174760. doi: 10.1371/journal.pone.0174760. eCollection 2017.
Identifying sociodemographic disparities in chemotherapy and hematopoietic cell transplantation (HCT) utilization for acute lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML) may improve survival for underserved populations. In this study, we incorporate neighborhood socioeconomic status (nSES), marital status, and distance from transplant center with previously studied factors to provide a comprehensive analysis of sociodemographic factors influencing treatments for ALL and AML.
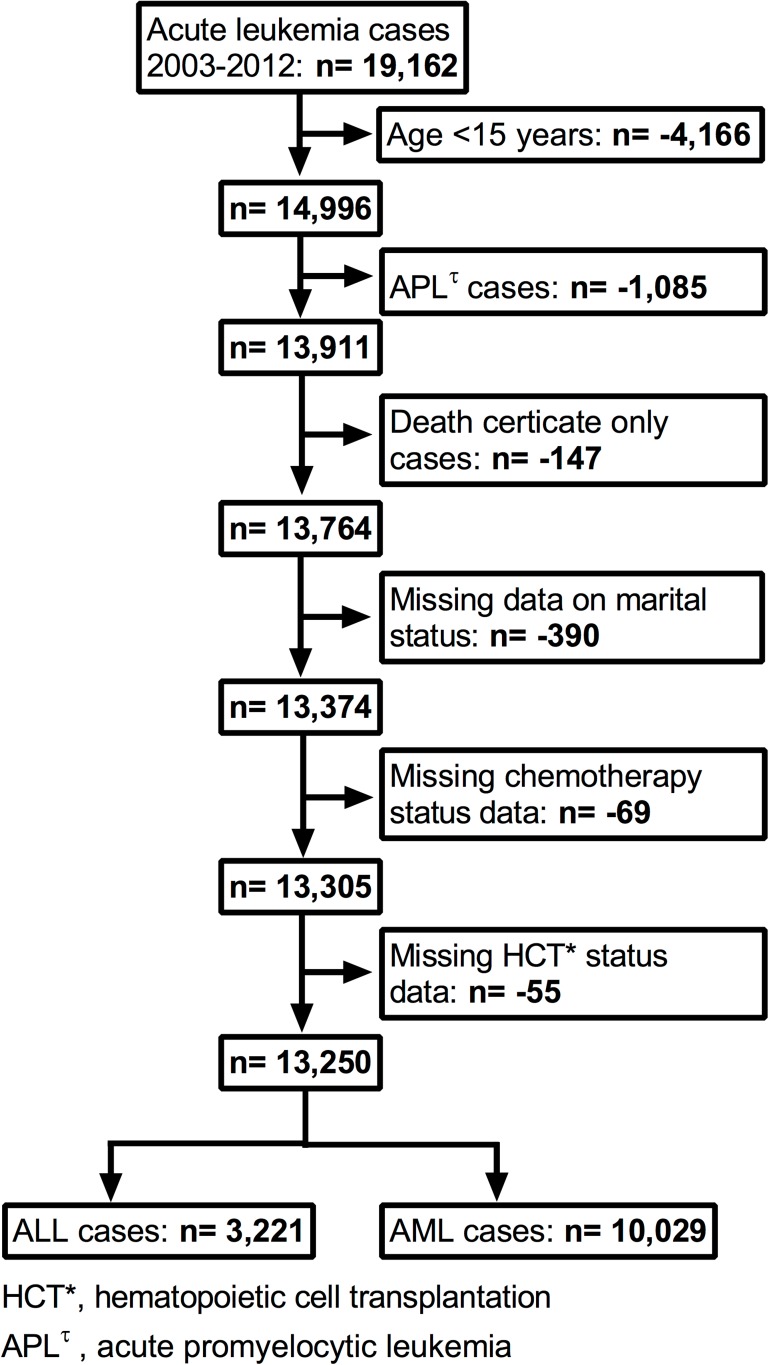
Using the California Cancer Registry, we performed a retrospective, population-based study of patients ≥15 years old with ALL (n = 3,221) or AML (n = 10,029) from 2003 through 2012. The effect of age, sex, race/ethnicity, marital status, nSES, and distance from nearest transplant center on receiving no treatment, chemotherapy alone, or chemotherapy then HCT was analyzed.
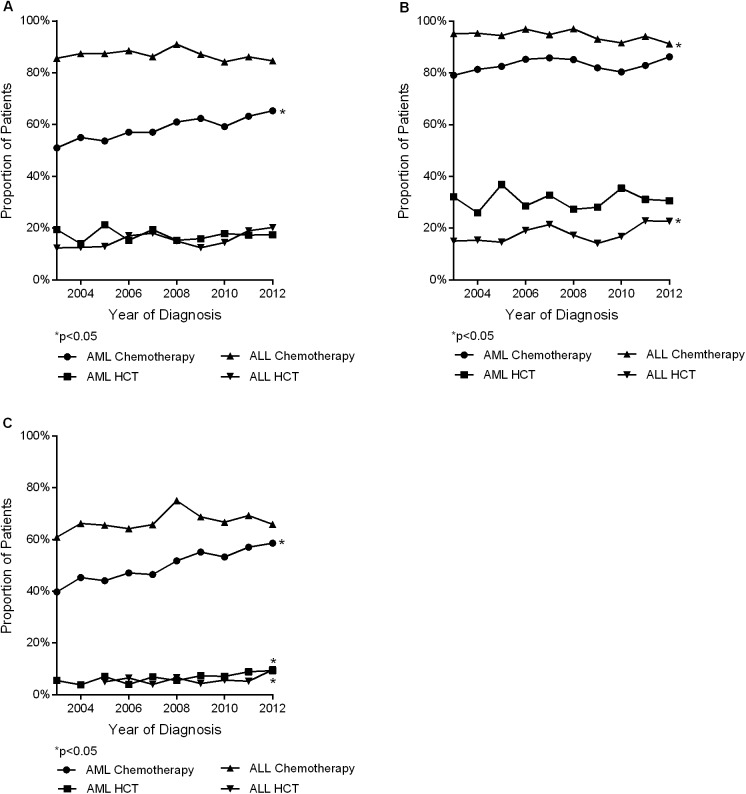
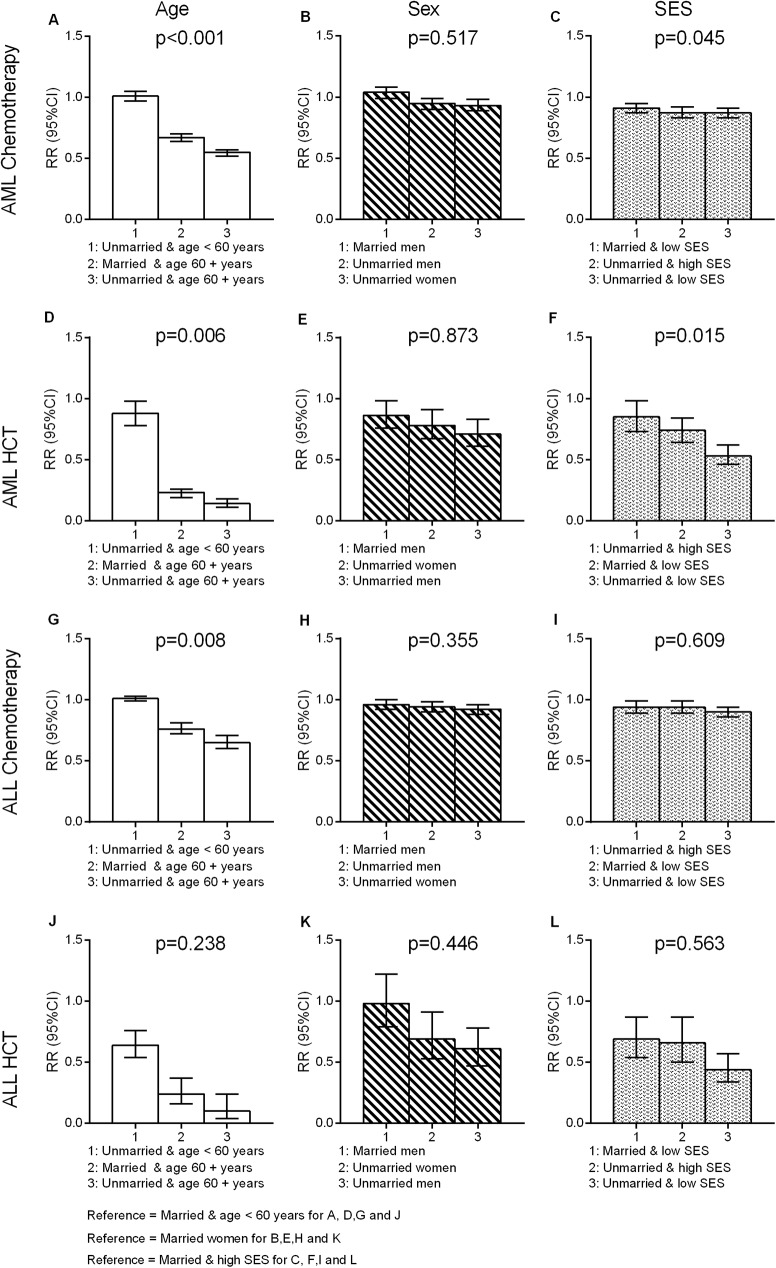
No treatment, chemotherapy alone, or chemotherapy then HCT were received by 11%, 75%, and 14% of ALL patients and 36%, 53%, and 11% of AML patients, respectively. For ALL patients ≥60 years old, HCT utilization increased from 5% in 2005 to 9% in 2012 (p = 0.03). For AML patients ≥60 years old, chemotherapy utilization increased from 39% to 58% (p<0.001) and HCT utilization from 5% to 9% from 2005 to 2012 (p<0.001). Covariate-adjusted analysis revealed decreasing relative risk (RR) of chemotherapy with increasing age for both ALL and AML (trend p <0.001). Relative to non-Hispanic whites, lower HCT utilization occurred in Hispanic [ALL, RR = 0.80 (95% CI = 0.65-0.98); AML, RR = 0.86 (95% CI = 0.75-0.99)] and non-Hispanic black patients [ALL, RR = 0.40 (95% CI = 0.18-0.89); AML, RR = 0.60 (95% CI = 0.44-0.83)]. Compared to married patients, never married patients had a lower RR of receiving chemotherapy [ALL, RR = 0.96 (95% CI = 0.92-0.99); AML, RR = 0.94 (95% CI = 0.90-0.98)] or HCT [ALL, RR = 0.58 (95% CI = 0.47-0.71); AML, RR = 0.80 (95% CI = 0.70-0.90)]. Lower nSES quintiles predicted lower chemotherapy and HCT utilization for both ALL and AML (trend p <0.001).
Older age, lower nSES, and being unmarried predicted lower utilization of chemotherapy and HCT among ALL and AML patients whereas having Hispanic or black race/ethnicity predicted lower rates of HCT. Addressing these disparities may increase utilization of curative therapies in underserved acute leukemia populations.
识别急性淋巴细胞白血病(ALL)和急性髓系白血病(AML)患者在化疗及造血细胞移植(HCT)使用方面的社会人口统计学差异,可能会提高医疗服务不足人群的生存率。在本研究中,我们将邻里社会经济地位(nSES)、婚姻状况以及与移植中心的距离纳入先前研究的因素中,以全面分析影响ALL和AML治疗的社会人口统计学因素。
利用加利福尼亚癌症登记处的数据,我们对2003年至2012年间年龄≥15岁的ALL患者(n = 3221)和AML患者(n = 10029)进行了一项基于人群的回顾性研究。分析了年龄、性别、种族/民族、婚姻状况、nSES以及与最近移植中心的距离对未接受任何治疗、仅接受化疗或先接受化疗后接受HCT的影响。
ALL患者中分别有11%、75%和14%未接受任何治疗、仅接受化疗或先接受化疗后接受HCT,AML患者中这一比例分别为36%、53%和11%。对于年龄≥60岁的ALL患者,HCT的使用率从2005年的5%增至2012年的9%(p = 0.03)。对于年龄≥60岁的AML患者,化疗使用率从2005年的39%增至2012年的58%(p<0.001),HCT使用率从5%增至9%(p<0.001)。协变量调整分析显示,ALL和AML患者化疗的相对风险(RR)均随年龄增长而降低(趋势p<0.001)。相对于非西班牙裔白人,西班牙裔患者[ALL,RR = 0.80(95%CI = 0.65 - 0.98);AML,RR = 0.86(95%CI = 0.75 - 0.99)]和非西班牙裔黑人患者[ALL,RR = 0.40(95%CI = 0.18 - 0.89);AML,RR = 0.60(95%CI = 0.44 - 0.83)]的HCT使用率较低。与已婚患者相比,未婚患者接受化疗[ALL,RR = 0.96(95%CI = 0.92 - 0.99);AML,RR = 0.94(95%CI = 0.90 - 0.98)]或HCT[ALL,RR = 0.58(95%CI = 0.47 - 0.71);AML,RR = 0.80(95%CI = 0.70 - 0.90)]的RR较低。较低的nSES五分位数预示着ALL和AML患者的化疗及HCT使用率较低(趋势p<0.001)。
年龄较大、nSES较低以及未婚预示着ALL和AML患者化疗及HCT的使用率较低,而西班牙裔或黑人种族/民族预示着HCT的使用率较低。解决这些差异可能会提高医疗服务不足的急性白血病人群中治愈性疗法的使用率。