Jagai Jyotsna S, Grossman Elena, Navon Livia, Sambanis Apostolis, Dorevitch Samuel
Division of Environmental and Occupational Health Sciences, School of Public Health, University of Illinois at Chicago, Chicago, USA.
Centers for Disease Control and Prevention, Illinois Department of Public Health, Chicago, USA.
Environ Health. 2017 Apr 7;16(1):38. doi: 10.1186/s12940-017-0245-1.
The disease burden due to heat-stress illness (HSI), which can result in significant morbidity and mortality, is expected to increase as the climate continues to warm. In the United States (U.S.) much of what is known about HSI epidemiology is from analyses of urban heat waves. There is limited research addressing whether HSI hospitalization risk varies between urban and rural areas, nor is much known about additional diagnoses of patients hospitalized for HSI.
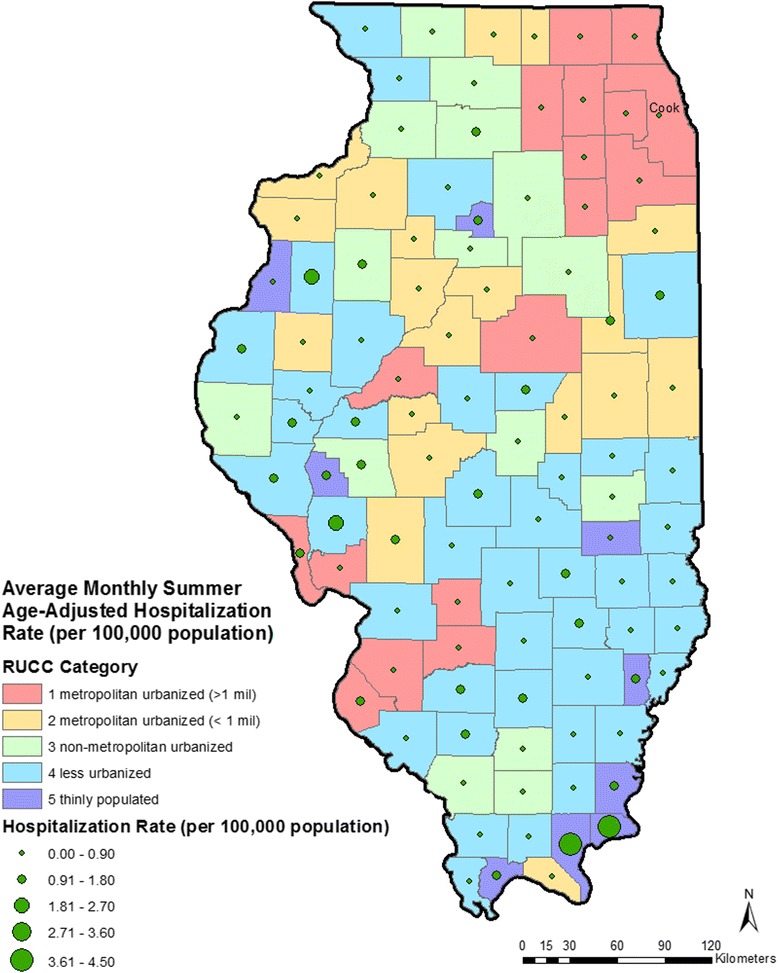
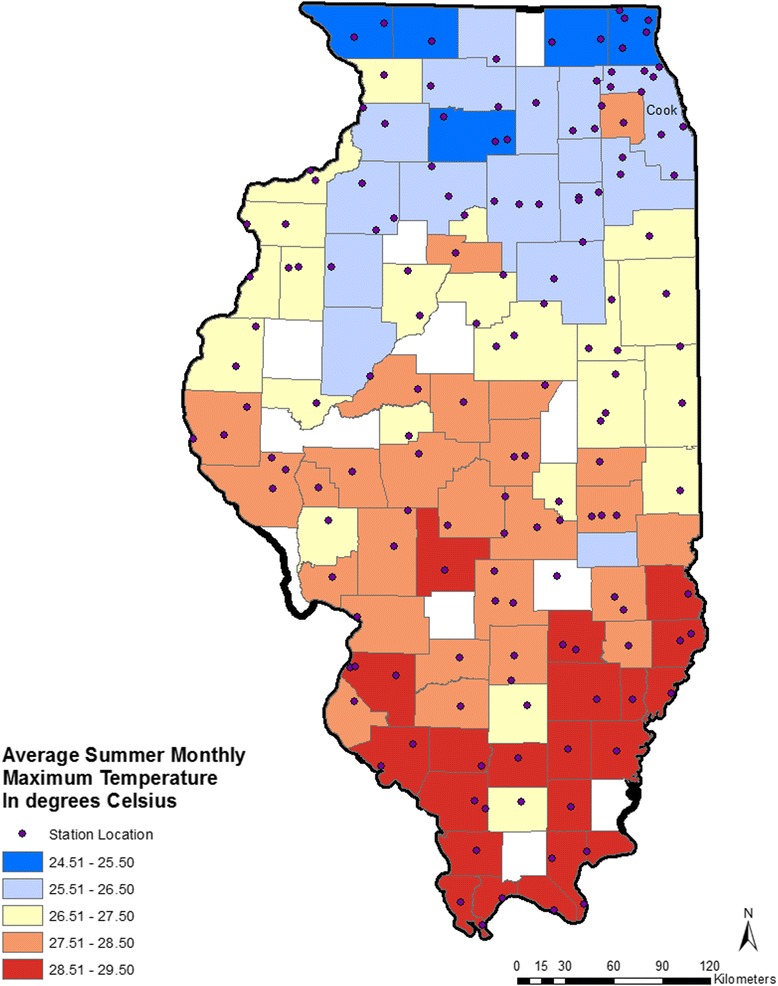
Hospitalizations in Illinois for HSI (ICD-9-CM codes 992.x or E900) in the months of May through September from 1987 to 2014 (n = 8667) were examined. Age-adjusted mean monthly hospitalization rates were calculated for each county using U.S. Census population data. Counties were categorized into five urban-rural strata using Rural Urban Continuum Codes (RUCC) (RUCC1, most urbanized to RUCC5, thinly populated). Average maximum monthly temperature (°C) was calculated for each county using daily data. Multi-level linear regression models were used, with county as the fixed effect and temperature as random effect, to model monthly hospitalization rates, adjusting for the percent of county population below the poverty line, percent of population that is Non-Hispanic Black, and percent of the population that is Hispanic. All analyses were stratified by county RUCC. Additional diagnoses of patients hospitalized for HSI and charges for hospitalization were summarized.
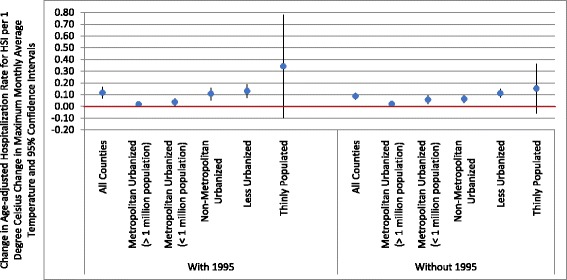
Highest rates of HSI hospitalizations were seen in the most rural, thinly populated stratum (mean annual summer hospitalization rate of 1.16 hospitalizations per 100,000 population in the thinly populated strata vs. 0.45 per 100,000 in the metropolitan urban strata). A one-degree Celsius increase in maximum monthly average temperature was associated with a 0.34 increase in HSI hospitalization rate per 100,000 population in the thinly populated counties compared with 0.02 per 100,000 in highly urbanized counties. The most common additional diagnoses of patients hospitalized with HSI were dehydration, electrolyte abnormalities, and acute renal disorders. Total and mean hospital charges for HSI cases were $167.7 million and $20,500 (in 2014 US dollars).
Elevated temperatures appear to have different impacts on HSI hospitalization rates as function of urbanization. The most rural and the most urbanized counties of Illinois had the largest increases in monthly hospitalization rates for HSI per unit increase in the average monthly maximum temperature. This suggests that vulnerability of communities to heat is complex and strategies to reduce HSI may need to be tailored to the degree of urbanization of a county.
热应激疾病(HSI)可导致显著的发病率和死亡率,随着气候持续变暖,其疾病负担预计会增加。在美国,关于HSI流行病学的许多知识来自对城市热浪的分析。关于HSI住院风险在城乡地区之间是否存在差异的研究有限,对于因HSI住院患者的其他诊断情况也了解甚少。
对1987年至2014年5月至9月期间伊利诺伊州因HSI(国际疾病分类第九版临床修正版编码992.x或E900)住院的病例(n = 8667)进行了研究。使用美国人口普查人口数据计算每个县的年龄调整后月平均住院率。利用农村城市连续编码(RUCC)(RUCC1,城市化程度最高到RUCC5,人口稀少)将各县分为五个城乡层次。使用每日数据计算每个县的月平均最高温度(摄氏度)。采用多水平线性回归模型,以县为固定效应,温度为随机效应,对月住院率进行建模,并对低于贫困线的县人口百分比、非西班牙裔黑人人口百分比以及西班牙裔人口百分比进行调整。所有分析均按县RUCC分层。总结了因HSI住院患者的其他诊断情况以及住院费用。
在人口最稀少的农村地区,HSI住院率最高(人口稀少层的年夏季平均住院率为每10万人中有1.16例住院,而大都市城区为每10万人中有0.45例)。月平均最高温度每升高1摄氏度,人口稀少县的HSI住院率每10万人增加0.34例,而高度城市化县每10万人增加0.02例。因HSI住院患者最常见的其他诊断为脱水、电解质异常和急性肾脏疾病。HSI病例的总住院费用和平均住院费用分别为1.677亿美元和20500美元(2014年美元)。
温度升高对HSI住院率的影响似乎因城市化程度而异。伊利诺伊州人口最稀少和城市化程度最高的县,月平均最高温度每升高1单位,HSI月住院率的增幅最大。这表明社区对高温的脆弱性很复杂,降低HSI的策略可能需要根据县的城市化程度进行调整。