Covella Michele, Rowin Ethan J, Hill Nicholas S, Preston Ioana R, Milan Alberto, Opotowsky Alexander R, Maron Barry J, Maron Martin S, Maron Bradley A
From the Division of Cardiology, Hypertrophic Cardiomyopathy Institute (M.C., E.J.R., B.J.M., M.S.M.) and Division of Pulmonary, Critical Care and Sleep Medicine (N.S.H., I.R.P.), Tufts Medical Center, Boston, MA; Division of Internal Medicine, Department of Medical Sciences, University of Torino, Italy (M.C., A.M.); Department of Pediatric Cardiology, Boston Children's Hospital, MA (A.R.O.); Division of Cardiovascular Medicine, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, MA (B.A.M.); and Department of Cardiology, Boston VA Healthcare System, MA (B.A.M.).
Circ Heart Fail. 2017 Apr;10(4):e003689. doi: 10.1161/CIRCHEARTFAILURE.116.003689.
There are limited data on the prevalence, pathophysiology, and management implications of pulmonary hypertension in patients with obstructive hypertrophic cardiomyopathy and advanced heart failure.
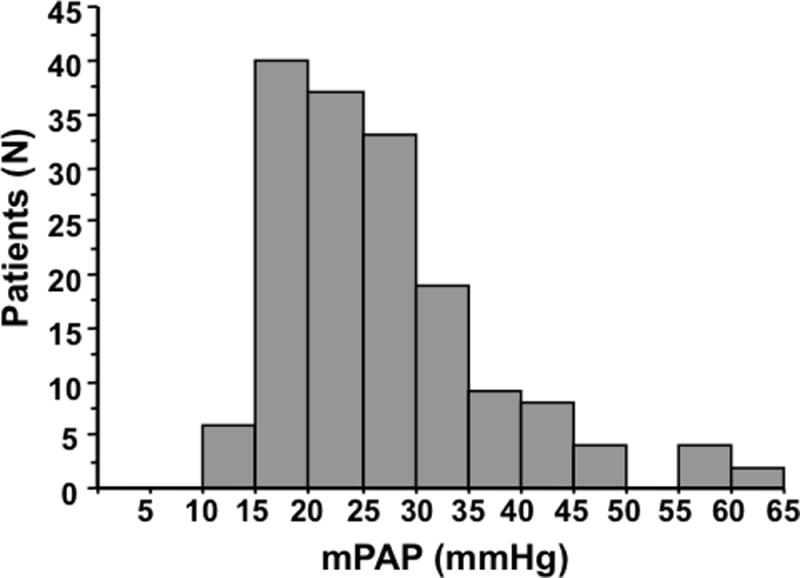
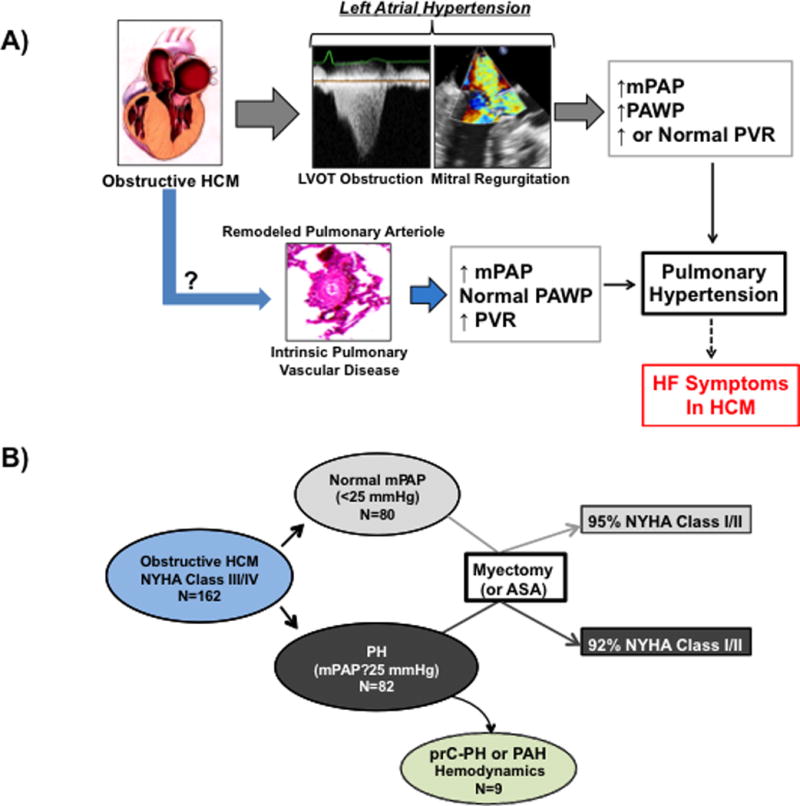
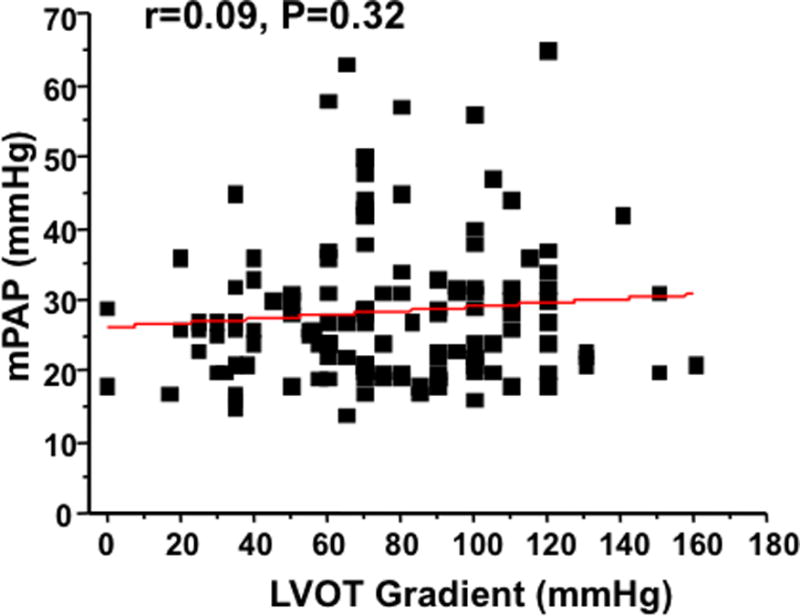
To assess the clinical significance of measured cardiopulmonary hemodynamics in hypertrophic cardiomyopathy patients with heart failure, we retrospectively assessed right heart catheterization data in 162 consecutive patients with outflow tract gradients (median [interquartile range], 90 mm Hg [70-110 mm Hg]), 59±11 years old, and 49% men, predominately New York Heart Association class III/IV status. Pulmonary hypertension (mean pulmonary artery pressure, ≥25 mm Hg) was present in 82 patients (51%), including 29 (18%) regarded as moderate-severe (mean pulmonary artery pressure, ≥35 mm Hg) and 28 (34%) also had increased pulmonary vascular resistance >3.0 WU. The pulmonary artery wedge pressure was ≤15 mm Hg in 54%, indicating that left atrial hypertension was absent in a majority of patients. Notably, 9 patients (11%) met hemodynamic criteria for precapillary pulmonary hypertension (mean pulmonary artery pressure, ≥25 mm Hg; pulmonary vascular resistance, >3.0 WU; pulmonary artery wedge pressure, ≤15 mm Hg). Over a median follow-up of 327 days (90-743 days) after surgical myectomy (or alcohol septal ablation), 92% and 95% of patients with or without preoperative pulmonary hypertension, respectively, were asymptomatic or mildly symptomatic. One postoperative death occurred in a 59-year-old woman with acute respiratory failure and mean pulmonary artery pressure of 65 mm Hg.
Pulmonary hypertension was common in obstructive hypertrophic cardiomyopathy patients with advanced heart failure. Although possibly a contributor to preoperative heart failure, pulmonary hypertension did not significantly influence clinical and surgical outcome. Notably, a novel patient subgroup was identified with resting invasive hemodynamics consistent with pulmonary vascular disease.
关于梗阻性肥厚型心肌病合并晚期心力衰竭患者肺动脉高压的患病率、病理生理学及管理意义的数据有限。
为评估肥厚型心肌病心力衰竭患者经测量的心肺血流动力学的临床意义,我们回顾性分析了162例连续患者的右心导管检查数据,这些患者存在流出道压力阶差(中位数[四分位间距],90 mmHg[70 - 110 mmHg]),年龄59±11岁,49%为男性,主要为纽约心脏协会Ⅲ/Ⅳ级状态。82例患者(51%)存在肺动脉高压(平均肺动脉压≥25 mmHg),其中29例(18%)为中重度(平均肺动脉压≥35 mmHg),28例(34%)肺血管阻力也升高>3.0 WU。54%的患者肺动脉楔压≤15 mmHg,表明大多数患者不存在左房高压。值得注意的是,9例患者(11%)符合毛细血管前性肺动脉高压的血流动力学标准(平均肺动脉压≥25 mmHg;肺血管阻力>3.0 WU;肺动脉楔压≤15 mmHg)。在手术心肌切除术(或酒精室间隔消融术)后中位随访327天(90 - 743天)期间,术前有或无肺动脉高压的患者分别有92%和95%无症状或症状轻微。1例59岁女性术后死亡,其患有急性呼吸衰竭,平均肺动脉压为65 mmHg。
肺动脉高压在梗阻性肥厚型心肌病合并晚期心力衰竭患者中很常见。尽管肺动脉高压可能是术前心力衰竭的一个促成因素,但它并未显著影响临床和手术结局。值得注意的是,我们识别出了一个新的患者亚组,其静息有创血流动力学与肺血管疾病一致。