Gao Jing, Perlman Alan, Kalache Safa, Berman Nathaniel, Seshan Surya, Salvatore Steven, Smith Lindsey, Wehrli Natasha, Waldron Levi, Kodali Hanish, Chevalier James
Department of Radiology, Weill Cornell Medicine, New York, New York, USA.
Rogosin Institute, New York Presbyterian Hospital, Weill Cornell Medicine, New York, New York, USA.
J Ultrasound Med. 2017 Nov;36(11):2245-2256. doi: 10.1002/jum.14209. Epub 2017 Apr 13.
To evaluate the value of multiparametric quantitative ultrasound imaging in assessing chronic kidney disease (CKD) using kidney biopsy pathologic findings as reference standards.
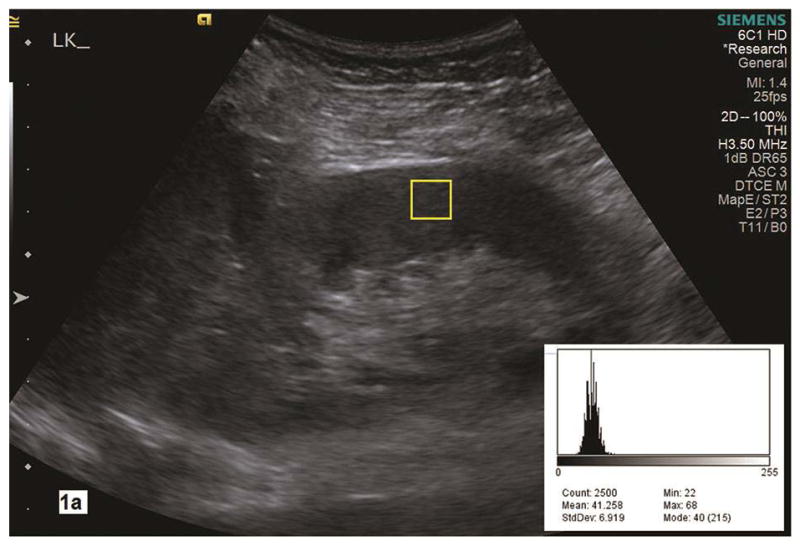
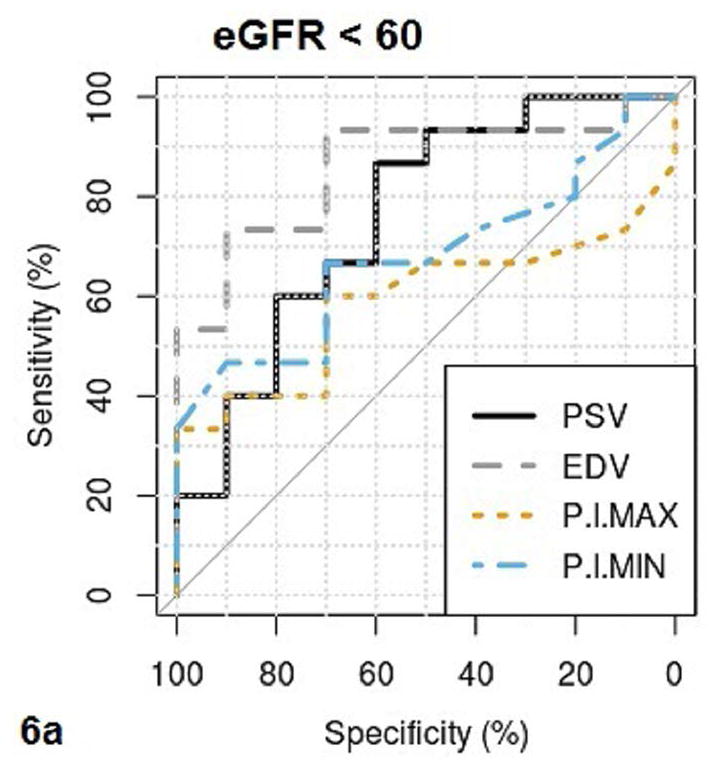
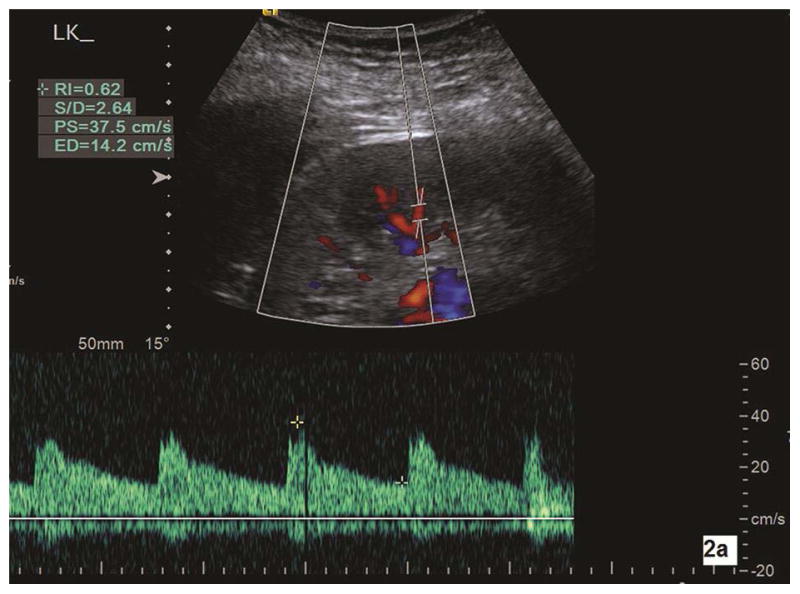
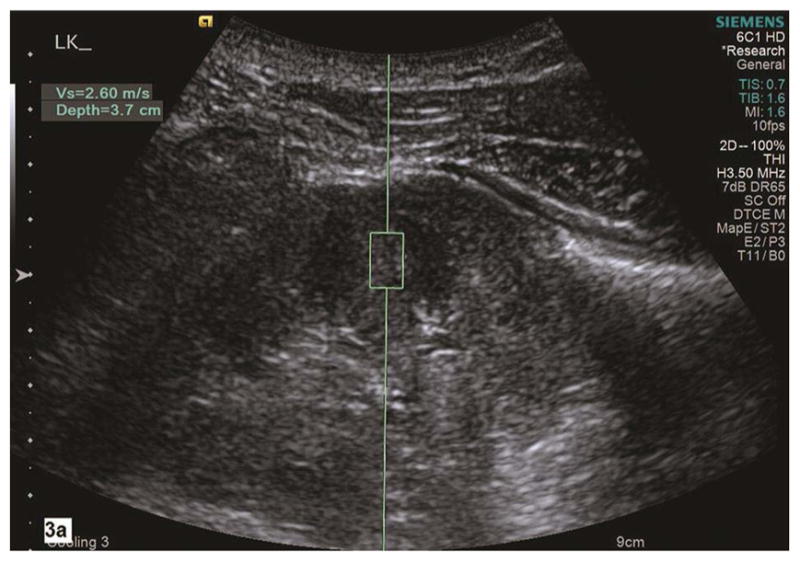
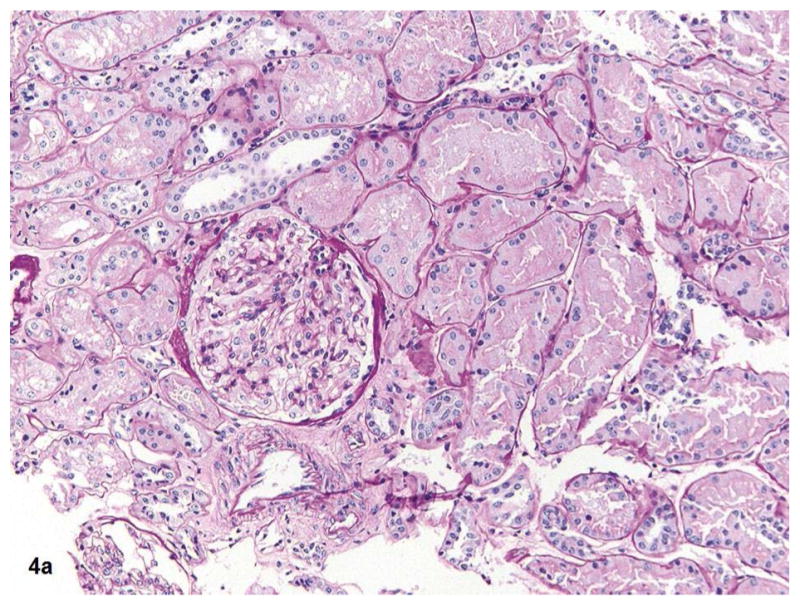
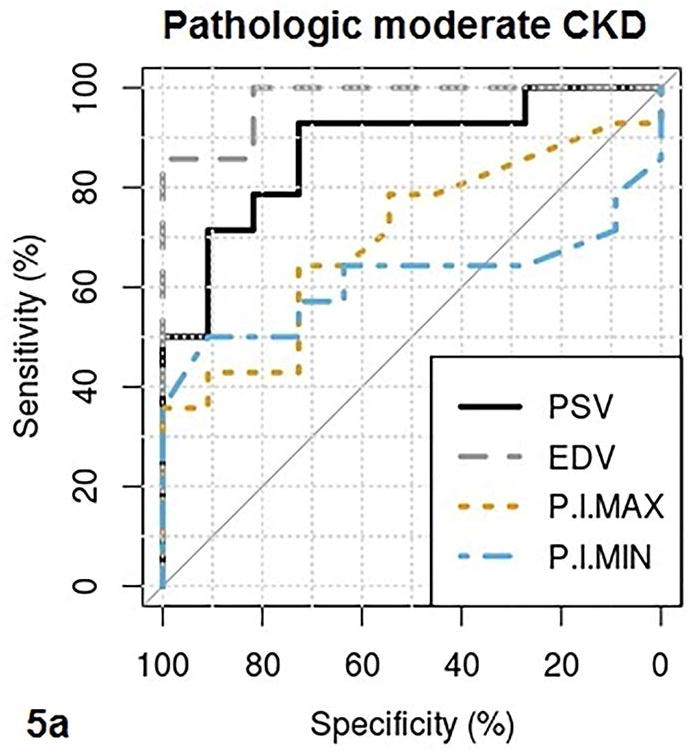
We prospectively measured multiparametric quantitative ultrasound markers with grayscale, spectral Doppler, and acoustic radiation force impulse imaging in 25 patients with CKD before kidney biopsy and 10 healthy volunteers. Based on all pathologic (glomerulosclerosis, interstitial fibrosis/tubular atrophy, arteriosclerosis, and edema) scores, the patients with CKD were classified into mild (no grade 3 and <2 of grade 2) and moderate to severe (at least 2 of grade 2 or 1 of grade 3) CKD groups. Multiparametric quantitative ultrasound parameters included kidney length, cortical thickness, pixel intensity, parenchymal shear wave velocity, intrarenal artery peak systolic velocity (PSV), end-diastolic velocity (EDV), and resistive index. We tested the difference in quantitative ultrasound parameters among mild CKD, moderate to severe CKD, and healthy controls using analysis of variance, analyzed correlations of quantitative ultrasound parameters with pathologic scores and the estimated glomerular filtration rate (GFR) using Pearson correlation coefficients, and examined the diagnostic performance of quantitative ultrasound parameters in determining moderate CKD and an estimated GFR of less than 60 mL/min/1.73 m using receiver operating characteristic curve analysis.
There were significant differences in cortical thickness, pixel intensity, PSV, and EDV among the 3 groups (all P < .01). Among quantitative ultrasound parameters, the top areas under the receiver operating characteristic curves for PSV and EDV were 0.88 and 0.97, respectively, for determining pathologic moderate to severe CKD, and 0.76 and 0.86 for estimated GFR of less than 60 mL/min/1.73 m . Moderate to good correlations were found for PSV, EDV, and pixel intensity with pathologic scores and estimated GFR.
The PSV, EDV, and pixel intensity are valuable in determining moderate to severe CKD. The value of shear wave velocity in assessing CKD needs further investigation.
以肾活检病理结果为参考标准,评估多参数定量超声成像在评估慢性肾脏病(CKD)中的价值。
我们前瞻性地对25例肾活检前的CKD患者和10名健康志愿者进行了多参数定量超声指标测量,采用灰阶、频谱多普勒和声学辐射力脉冲成像技术。根据所有病理(肾小球硬化、间质纤维化/肾小管萎缩、动脉硬化和水肿)评分,将CKD患者分为轻度(无3级且2级少于2个)和中重度(至少2个2级或1个3级)CKD组。多参数定量超声参数包括肾长、皮质厚度、像素强度、实质剪切波速度、肾内动脉收缩期峰值速度(PSV)、舒张末期速度(EDV)和阻力指数。我们使用方差分析检验轻度CKD、中重度CKD和健康对照之间定量超声参数的差异,使用Pearson相关系数分析定量超声参数与病理评分及估计肾小球滤过率(GFR)的相关性,并使用受试者工作特征曲线分析检验定量超声参数在确定中度CKD和估计GFR小于60 mL/min/1.73 m²方面的诊断性能。
三组之间的皮质厚度、像素强度、PSV和EDV存在显著差异(均P < 0.01)。在定量超声参数中,PSV和EDV在确定病理中重度CKD时受试者工作特征曲线下的最大面积分别为0.88和0.97,在估计GFR小于60 mL/min/1.73 m²时分别为0.76和0.86。发现PSV、EDV和像素强度与病理评分及估计GFR之间存在中度到良好的相关性。
PSV、EDV和像素强度在确定中重度CKD方面具有价值。剪切波速度在评估CKD中的价值需要进一步研究。