Sawai Toyomitsu, Nakao Takumi, Yamaguchi Shota, Yoshioka Sumako, Matsuo Nobuko, Suyama Naofumi, Yanagihara Katsunori, Mukae Hiroshi
Department of Respiratory Medicine, Nagasaki Harbor Medical Center City Hospital, 6-39 Shinchi-machi, Nagasaki, 850-8555, Japan.
Department of Laboratory Medicine, Nagasaki Harbor Medical Center City Hospital, 6-39 Shinchi-machi, Nagasaki, Japan.
BMC Infect Dis. 2017 Apr 13;17(1):272. doi: 10.1186/s12879-017-2370-4.
β-D-glucan (BDG) is a helpful diagnostic marker for many invasive fungal infections, but not for nocardiosis. Here, we reported the first case of nocardial infection with high serum level of BDG.
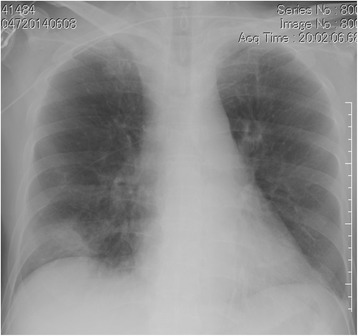
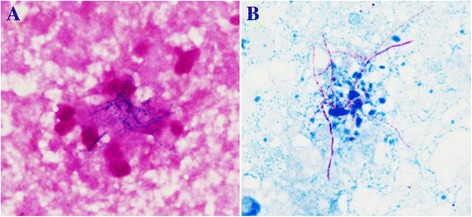
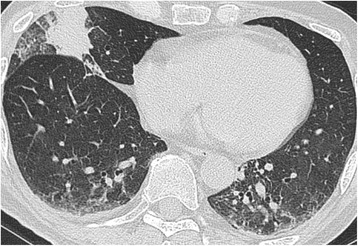
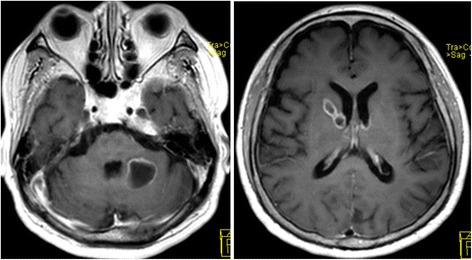
A 73-year-old man was hospitalized because of fever, headache, and appetite loss after 10 months of steroid and immunosuppressive therapy for cryptogenic organizing pneumonia. With a diagnosis of bacterial pneumonia, treatment with ampicillin/sulbactam was initiated. There was improvement on chest radiograph, but fever persisted. Further work-up revealed multiple brain abscesses on cranial magnetic resonance imaging (MRI). Serum galactomannan and BDG were elevated at 0.6 index and 94.7 pg/ml, respectively. Voriconazole was initiated for presumed aspergillus brain abscess. However, fever persisted and consciousness level deteriorated. Drainage of brain abscess was performed; based on the Gram stain and Kinyoun acid-fast stain, disseminated nocardiosis was diagnosed. Voriconazole was then shifter to trimethoprim/sulfamethoxazole. The presence of Nocardia farcinica was confirmed by the 16S rRNA gene sequence. Treatment course was continued; BDG level normalized after 1 month and cranial MRI showed almost complete improvement after 2 months.
BDG assay is widely used to diagnose invasive fungal infection; therefore, clinicians should be aware that Nocardia species may show cross-reactivity with BDG assay on serum.
β-D-葡聚糖(BDG)是许多侵袭性真菌感染的有用诊断标志物,但对诺卡菌病无效。在此,我们报告了首例血清BDG水平升高的诺卡菌感染病例。
一名73岁男性因隐源性机化性肺炎接受10个月的类固醇和免疫抑制治疗后,出现发热、头痛和食欲减退而住院。诊断为细菌性肺炎,开始使用氨苄西林/舒巴坦治疗。胸部X线片有所改善,但发热持续。进一步检查发现头颅磁共振成像(MRI)显示多发脑脓肿。血清半乳甘露聚糖和BDG分别升高至0.6指数和94.7 pg/ml。因推测为曲霉性脑脓肿开始使用伏立康唑治疗。然而,发热持续,意识水平恶化。进行了脑脓肿引流;根据革兰氏染色和金胺O抗酸染色,诊断为播散性诺卡菌病。然后将伏立康唑改为复方磺胺甲恶唑。通过16S rRNA基因序列确认了豚鼠耳炎诺卡菌的存在。继续治疗过程;1个月后BDG水平恢复正常,2个月后头颅MRI显示几乎完全改善。
BDG检测广泛用于诊断侵袭性真菌感染;因此,临床医生应意识到诺卡菌属可能与血清BDG检测存在交叉反应。