Leligdowicz Aleksandra, Conroy Andrea L, Hawkes Michael, Zhong Kathleen, Lebovic Gerald, Matthay Michael A, Kain Kevin C
Department of Medicine, University of Toronto, Toronto, Canada.
Sandra A. Rotman Laboratories, Sandra Rotman Centre for Global Health, University Health Network, Toronto, Canada.
PLoS One. 2017 Apr 18;12(4):e0175130. doi: 10.1371/journal.pone.0175130. eCollection 2017.
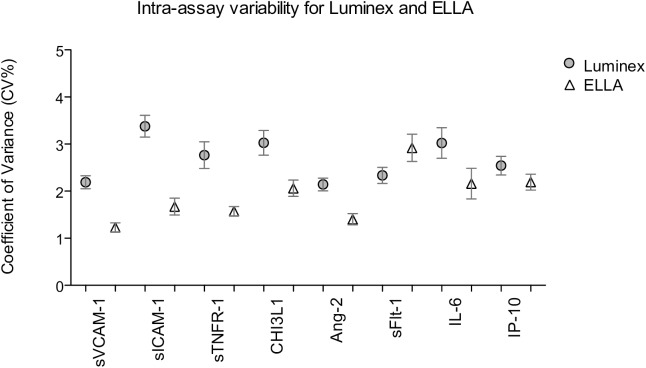
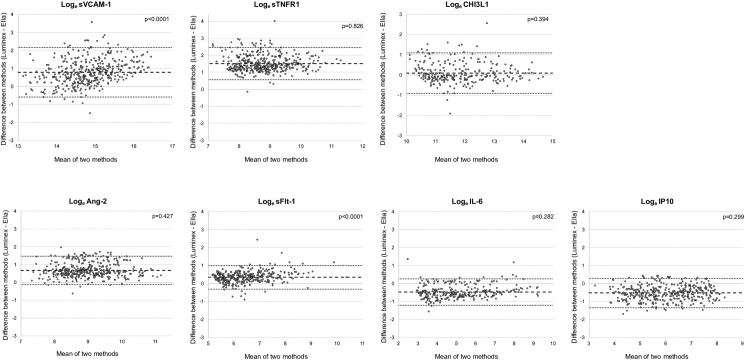
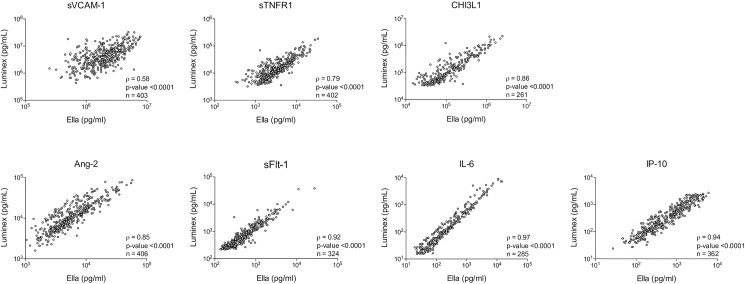
Biomarkers can prognosticate outcome and enable risk-stratification. In severe infection, focusing on multiple markers reflecting pathophysiological mechanisms of organ injury could enhance management and pathway-directed therapeutics. Limited data exist on the performance of multiplex biomarker platforms. Our goal was to compare endothelial and immune activation biomarkers in severe pediatric infections using two multiplex platforms. Frozen plasma from 410 children presenting to the Jinja Regional Hospital in Uganda with suspected infection was used to measure biomarkers of endothelial (Angiopoietin-2, sFlt-1, sVCAM-1, sICAM-1) and immune (IL-6, IP-10, sTNFR-1, CHI3L1) activation. Two multiplex platforms (Luminex®, EllaTM) based on monoclonal antibody sandwich immunoassays using biotin-streptavidin conjugate chemistry were selected with reagents from R&D Systems. The two platforms differed in ease and time of completion, number of samples per assay, and dynamic concentration range. Intra-assay variability assessed using a coefficient of variation (CV%) was 2.2-3.4 for Luminex® and 1.2-2.9 for EllaTM. Correlations for biomarker concentrations within dynamic range of both platforms were best for IL-6 (ρ = 0.96, p<0.0001), IP-10 (ρ = 0.94, p<0.0001) and sFlt-1 (ρ = 0.94, p<0.0001). Agreement between concentrations obtained by both methods assessed by the Bland-Altman test varied, with best agreement for CHI3L1. Our data suggest that biomarkers of endothelial and immune activation can be readily measured with multiplex platforms. Luminex® and EllaTM produced reliable results with excellent CV% values. The EllaTM platform was more automated and completed in 75 minutes, potentially compatible with near-patient use. Trends in concentrations obtained by these methods were highly correlated, although absolute values varied, suggesting caution is required when comparing data from different multiplex platforms.
生物标志物可以预测预后并实现风险分层。在严重感染中,关注反映器官损伤病理生理机制的多种标志物可以加强管理和实施针对特定途径的治疗。关于多重生物标志物平台性能的数据有限。我们的目标是使用两种多重平台比较严重儿科感染中的内皮和免疫激活生物标志物。从乌干达金贾地区医院就诊的410名疑似感染儿童中采集的冻存血浆用于测量内皮(血管生成素-2、可溶性血管内皮生长因子受体-1、可溶性血管细胞黏附分子-1、可溶性细胞间黏附分子-1)和免疫(白细胞介素-6、干扰素诱导蛋白10、可溶性肿瘤坏死因子受体-1、几丁质酶3样蛋白1)激活的生物标志物。选用了基于单克隆抗体夹心免疫测定法、使用生物素-链霉亲和素共轭化学的两种多重平台(Luminex®、EllaTM)以及来自研发系统公司的试剂。这两种平台在操作简便程度、完成时间、每次检测的样本数量和动态浓度范围方面存在差异。使用变异系数(CV%)评估的批内变异在Luminex®平台上为2.2 - 3.4,在EllaTM平台上为1.2 - 2.9。在两种平台的动态范围内,生物标志物浓度的相关性对于白细胞介素-6(ρ = 0.96,p<0.0001)、干扰素诱导蛋白10(ρ = 0.94,p<0.0001)和可溶性血管内皮生长因子受体-1(ρ = 0.94,p<0.0001)最佳。通过布兰德-奥特曼检验评估的两种方法所获浓度之间的一致性各不相同,几丁质酶3样蛋白1的一致性最佳。我们的数据表明,内皮和免疫激活的生物标志物可以通过多重平台轻松测量。Luminex®和EllaTM平台产生了可靠的结果,CV%值优异。EllaTM平台自动化程度更高,75分钟即可完成检测,可能适用于床旁检测。尽管绝对值有所不同,但通过这些方法获得的浓度趋势高度相关,这表明在比较来自不同多重平台的数据时需要谨慎。