Shi Keda, Shen Zeren, Zhu Guiqi, Meng Fansheng, Gu Mengli, Ji Feng
Department of Gastroenterology, The First Affiliated Hospital, School of Medicine, Zhejiang University, No. 79 Qingchun Rd, Hangzhou, 310000, Zhejiang, China.
Eye Center, The Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China.
BMC Gastroenterol. 2017 Apr 19;17(1):55. doi: 10.1186/s12876-017-0610-0.
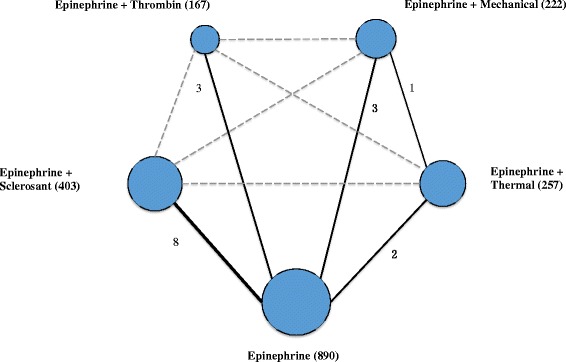
Adding a second endoscopic therapy to epinephrine injection might improve hemostatic efficacy in patients with high-risk bleeding ulcers but the optimum modality remains unknown. We aimed to estimate the comparative efficacy of different dual endoscopic therapies for the management of bleeding peptic ulcers through random-effects Bayesian network meta-analysis.
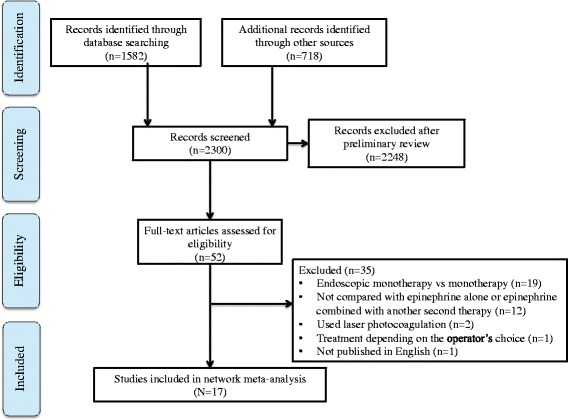
Different databases were searched for controlled trials comparing dual therapy versus epinephrine monotherapy or epinephrine combined with another second modality until September, 30 2016. We estimated the ORs for rebleeding, surgery and mortality among different treatments. Adverse events were also evaluated.
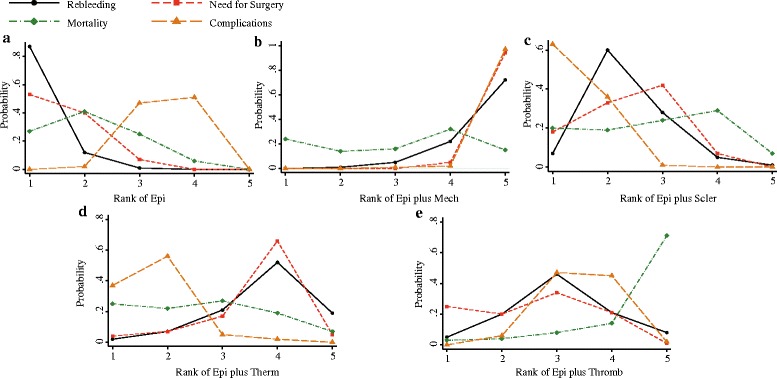
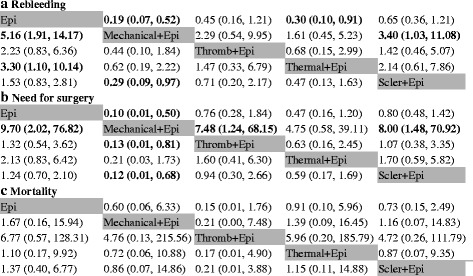
Seventeen eligible articles were included in the network meta-analysis. The addition of mechanical therapy (OR 0.19, 95% CrI 0.07-0.52 and OR 0.10, 95% CrI 0.01-0.50, respectively) after epinephrine injection significantly reduced the probability of rebleeding and surgery. Similarly, patients who received epinephrine plus thermal therapy showed a significantly decreased rebleeding rate (OR 0.30, 95% CrI 0.10-0.91), as well as a non-significant reduction in surgery (OR 0.47, 95% CrI 0.16-1.20). Although differing, epinephrine plus mechanical therapy did not provide a significant reduction in rebleeding (OR 0.62, 95% CrI 0.19-2.22) and surgery (OR 0.21, 95% CrI 0.03-1.73) compared to epinephrine plus thermal therapy. Sclerosant failed to confer further benefits and was ranked highest among the 5 treatments in relation to adverse events.
Mechanical therapy was the most appropriate modality to add to epinephrine injection. Epinephrine plus thermal coagulation was effective for controlling high risk bleeding ulcers. There was no further benefit with sclerosants with regard to rebleeding or surgery, and sclerosants were also associated with more adverse events than any other modality.
在肾上腺素注射基础上增加第二种内镜治疗方法可能会提高高危出血性溃疡患者的止血效果,但最佳治疗方式仍不明确。我们旨在通过随机效应贝叶斯网络荟萃分析评估不同双重内镜治疗方法对消化性溃疡出血的治疗效果。
检索不同数据库,查找比较双重治疗与肾上腺素单一疗法或肾上腺素联合另一种第二种治疗方法的对照试验,检索截至2016年9月30日。我们估算了不同治疗方法的再出血、手术及死亡率的比值比。同时也对不良事件进行了评估。
网络荟萃分析纳入了17篇符合条件的文章。肾上腺素注射后加用机械治疗(比值比分别为0.19,95%可信区间0.07 - 0.52和0.10,95%可信区间0.01 - 0.50)可显著降低再出血和手术概率。同样,接受肾上腺素加热凝治疗的患者再出血率显著降低(比值比0.30,95%可信区间0.10 - 0.91),手术率也有非显著性降低(比值比0.47,95%可信区间0.16 - 1.20)。尽管有所不同,但与肾上腺素加用热凝治疗相比,肾上腺素加用机械治疗在再出血(比值比0.62,95%可信区间0.19 - 2.22)和手术(比值比0.21,95%可信区间0.03 - 1.73)方面并未显著降低。硬化剂未能带来更多益处,且在5种治疗方法中不良事件发生率最高。
机械治疗是肾上腺素注射基础上最适宜添加的治疗方式。肾上腺素加用热凝治疗对控制高危出血性溃疡有效。硬化剂在再出血或手术方面未带来更多益处,且与其他任何治疗方式相比,硬化剂还与更多不良事件相关。