Department of Gastroenterology, The First Affiliated Hospital of Nanchang University, 17 Yongwaizheng, Street, Nanchang, 330006, Jiangxi Province, China.
BMC Gastroenterol. 2022 Jul 31;22(1):368. doi: 10.1186/s12876-022-02448-x.
Although the current guidelines recommend endoscopic combination therapy, endoscopic epinephrine injection (EI) monotherapy is still a simple, common and effective modality for treating peptic ulcer bleeding (PUB). However, the rebleeding risk after EI monotherapy is still high, and identifying rebleeding patients after EI monotherapy is unclear, which is highly important in clinical practice. This study aimed to identify risk factors and constructed a predictive nomogram related to rebleeding after EI monotherapy.
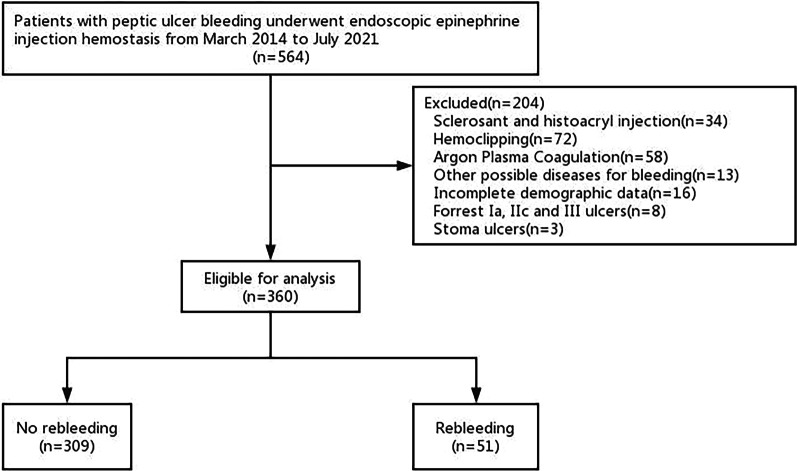
We consecutively and retrospectively analyzed 360 PUB patients who underwent EI monotherapy between March 2014 and July 2021 in our center. Then we identified independent risk factors associated with rebleeding after initial endoscopic EI monotherapy by multivariate logistic regression. A predictive nomogram was developed and validated based on the above predictors.
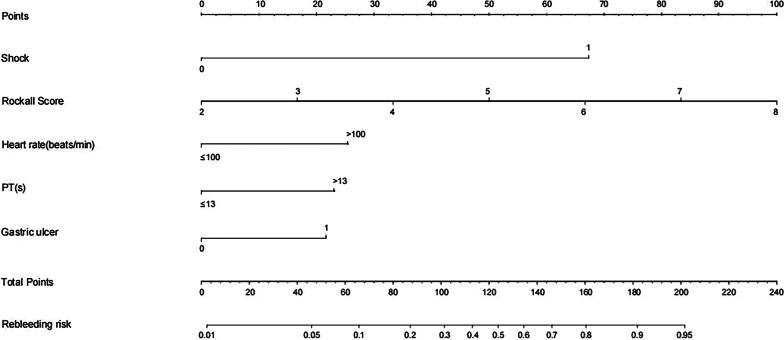
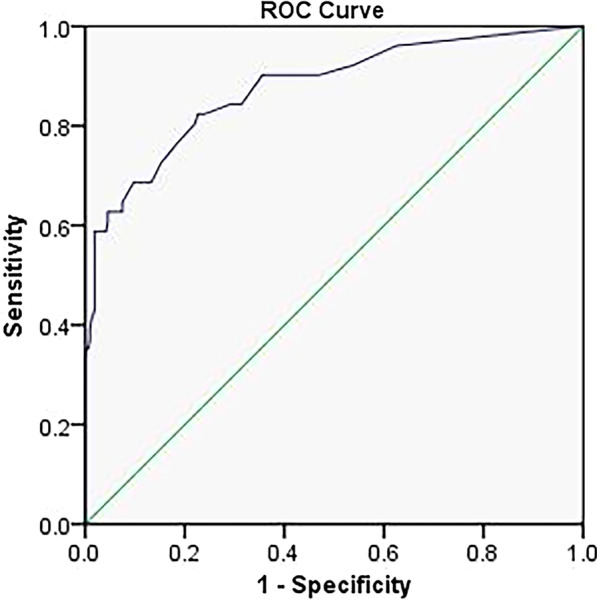
Among all PUB patients enrolled, 51 (14.2%) had recurrent hemorrhage within 30 days after endoscopic EI monotherapy. After multivariate logistic regression, shock [odds ratio (OR) = 12.691, 95% confidence interval (CI) 5.129-31.399, p < 0.001], Rockall score (OR = 1.877, 95% CI 1.250-2.820, p = 0.002), tachycardia (heart rate > 100 beats/min) (OR = 2.610, 95% CI 1.098-6.203, p = 0.030), prolonged prothrombin time (PT > 13 s) (OR = 2.387, 95% CI 1.019-5.588, p = 0.045) and gastric ulcer (OR = 2.258, 95% CI 1.003-5.084, p = 0.049) were associated with an increased risk of rebleeding after an initial EI monotherapy treatment. A nomogram incorporating these independent high-risk factors showed good discrimination, with an area under the receiver operating characteristic curve (AUROC) of 0.876 (95% CI 0.817-0.934) (p < 0.001).
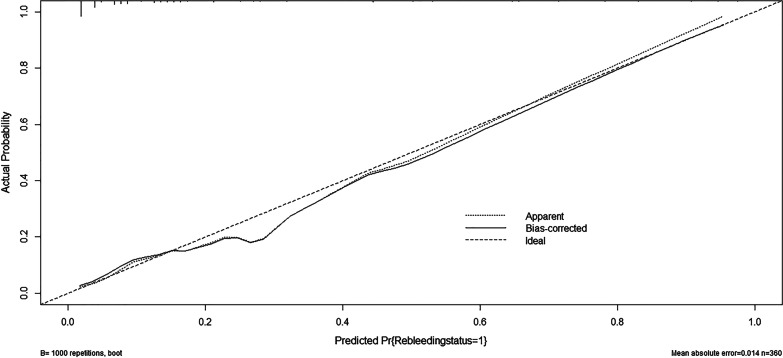
We developed a predictive nomogram of rebleeding after EI monotherapy, which had excellent prediction accuracy. This predictive nomogram can be conveniently used to identify low-risk rebleeding patients after EI monotherapy, allowing for decision-making in a clinical setting.
尽管目前的指南推荐内镜联合治疗,但内镜肾上腺素注射(EI)单药治疗仍是治疗消化性溃疡出血(PUB)的一种简单、常见且有效的方法。然而,EI 单药治疗后的再出血风险仍然较高,并且 EI 单药治疗后再出血患者的识别尚不清楚,这在临床实践中非常重要。本研究旨在确定与 EI 单药治疗后再出血相关的危险因素,并构建相关预测列线图。
我们连续回顾性分析了 2014 年 3 月至 2021 年 7 月期间在我院接受 EI 单药治疗的 360 例 PUB 患者。然后,我们通过多变量逻辑回归确定与初始内镜 EI 单药治疗后再出血相关的独立危险因素。根据上述预测因子,建立并验证了预测列线图。
所有纳入的 PUB 患者中,有 51 例(14.2%)在 EI 内镜单药治疗后 30 天内再次出现出血。多变量逻辑回归后,休克[比值比(OR)=12.691,95%置信区间(CI)5.129-31.399,p<0.001]、Rockall 评分(OR=1.877,95%CI 1.250-2.820,p=0.002)、心动过速(心率>100 次/分)(OR=2.610,95%CI 1.098-6.203,p=0.030)、延长的凝血酶原时间(PT>13s)(OR=2.387,95%CI 1.019-5.588,p=0.045)和胃溃疡(OR=2.258,95%CI 1.003-5.084,p=0.049)与 EI 单药初始治疗后再出血风险增加相关。纳入这些独立高危因素的列线图显示出良好的区分度,其受试者工作特征曲线下面积(AUROC)为 0.876(95%CI 0.817-0.934)(p<0.001)。
我们开发了一种 EI 单药治疗后再出血的预测列线图,具有良好的预测准确性。该预测列线图可方便地用于识别 EI 单药治疗后低风险再出血患者,为临床决策提供依据。