1 Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, The Netherlands.
2 Netherlands Heart Institute, The Netherlands.
Eur J Prev Cardiol. 2018 Apr;25(6):642-650. doi: 10.1177/2047487317752948. Epub 2018 Feb 7.
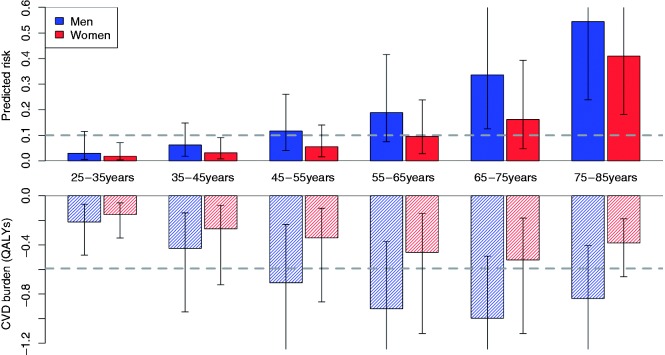
Background Cardiovascular disease (CVD) prevention is commonly focused on providing individuals at high predicted CVD risk with preventive medication. Whereas CVD risk increases rapidly with age, current risk-based selection of individuals mainly targets the elderly. However, the lifelong (preventable) consequences of CVD events may be larger in younger individuals. The purpose of this paper is to investigate if health benefits from preventive treatment may increase when the selection strategy is further optimised. Methods Data from three Dutch cohorts were combined ( n = 47469, men:women 1:1.92) and classified into subgroups based on age and gender. The Framingham global risk score was used to estimate 10-year CVD risk. The associated lifelong burden of CVD events according to this 10-year CVD risk was expressed as quality-adjusted life years lost. Based on this approach, the additional health benefits from preventive treatment, reducing this 10-year CVD risk, from selecting individuals based on their expected CVD burden rather than their expected CVD risk were estimated. These benefits were expressed as quality-adjusted life years gained over lifetime. Results When using the current selection strategy (10% risk threshold), 32% of the individuals were selected for preventive treatment. When the same proportion was selected based on burden, more younger and fewer older individuals would receive treatment. Across all individuals, the gain in quality-adjusted life years was 217 between the two strategies, over a 10-year time horizon. In addition, when combining the strategies 5% extra eligible individuals were selected resulting in a gain of 628 quality-adjusted life years. Conclusion Improvement of the selection approach of individuals can help to reduce further the CVD burden. Selecting individuals for preventive treatment based on their expected CVD burden will provide more younger and fewer older individuals with treatment, and will reduce the overall CVD burden.
心血管疾病(CVD)的预防通常侧重于为高预测 CVD 风险的个体提供预防性药物。虽然 CVD 风险随着年龄的增长而迅速增加,但目前基于风险的个体选择主要针对老年人。然而,CVD 事件的终身(可预防)后果在年轻人中可能更大。本文旨在研究当选择策略进一步优化时,预防性治疗的健康益处是否会增加。
合并了来自三个荷兰队列的数据(n=47469,男女比例为 1:1.92),并根据年龄和性别将其分为亚组。使用 Framingham 全球风险评分估计 10 年 CVD 风险。根据该 10 年 CVD 风险,CVD 事件的终身负担表示为丧失的质量调整生命年。基于这种方法,从基于个体预期 CVD 负担而不是预期 CVD 风险选择个体的角度,估计了预防治疗降低这 10 年 CVD 风险所带来的额外健康益处。这些益处表示为终生获得的质量调整生命年。
当使用当前的选择策略(10%风险阈值)时,32%的个体被选择进行预防性治疗。当根据负担选择相同比例时,更多的年轻个体和更少的老年个体将接受治疗。在所有个体中,两种策略之间的质量调整生命年增加了 217 年,时间范围为 10 年。此外,当结合这两种策略时,额外选择了 5%的合格个体,导致质量调整生命年增加了 628 年。
改进个体选择方法可以帮助进一步降低 CVD 负担。根据预期 CVD 负担选择个体进行预防性治疗将为更多的年轻个体和更少的老年个体提供治疗,并降低整体 CVD 负担。