Department of Experimental Pneumology and Allergology, Saarland University Faculty of Medicine, Homburg/Saar, Germany.
Department of Biometry, Epidemiology and Clinical informatics, Saarland University Faculty of Medicine, Homburg/Saar, Germany.
NPJ Prim Care Respir Med. 2017 Apr 21;27(1):28. doi: 10.1038/s41533-017-0026-x.
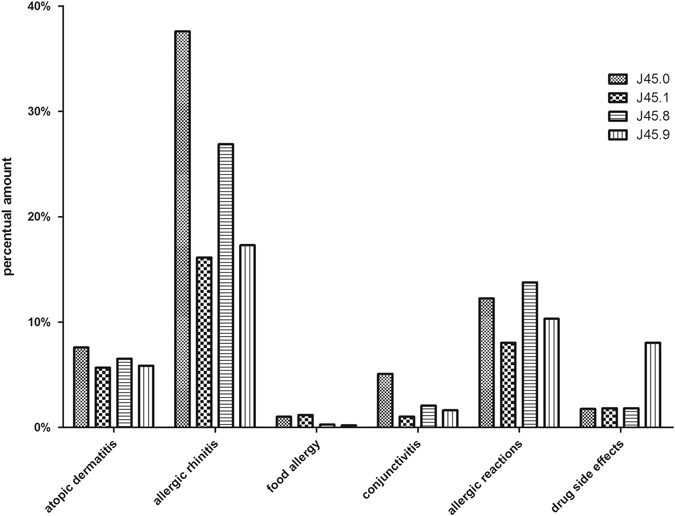
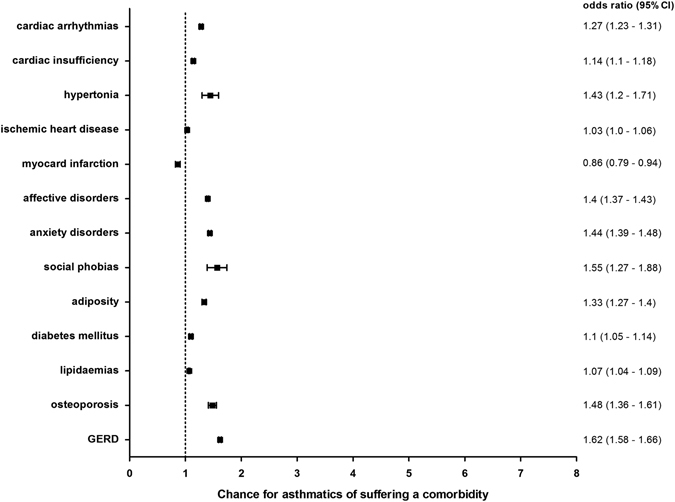
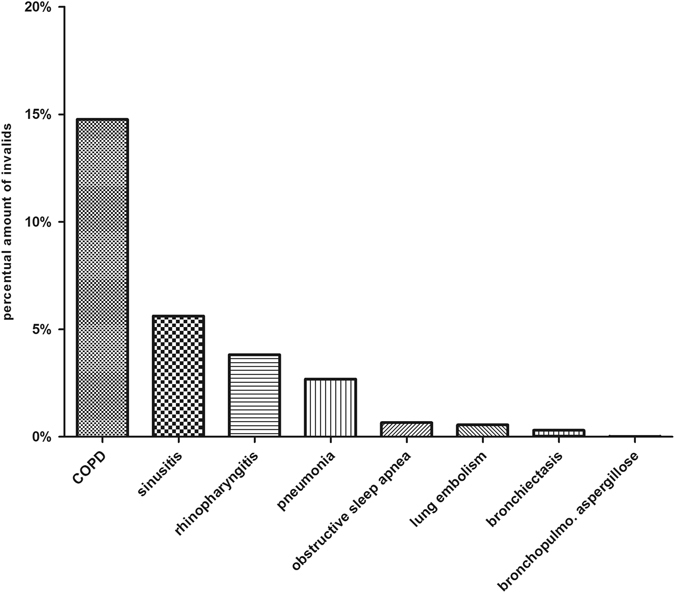
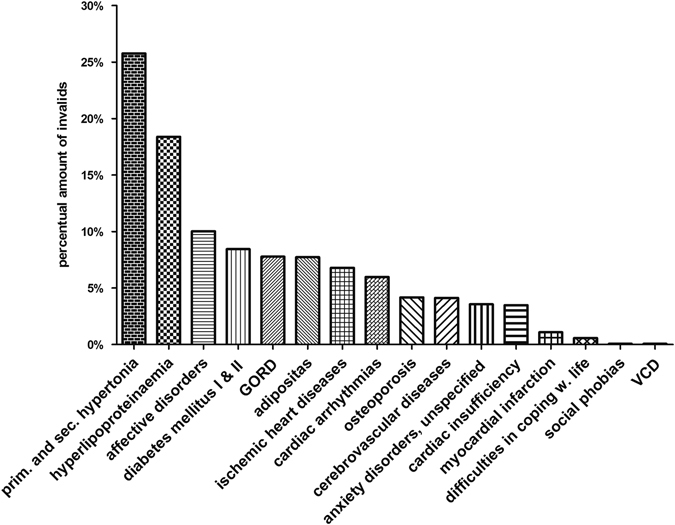
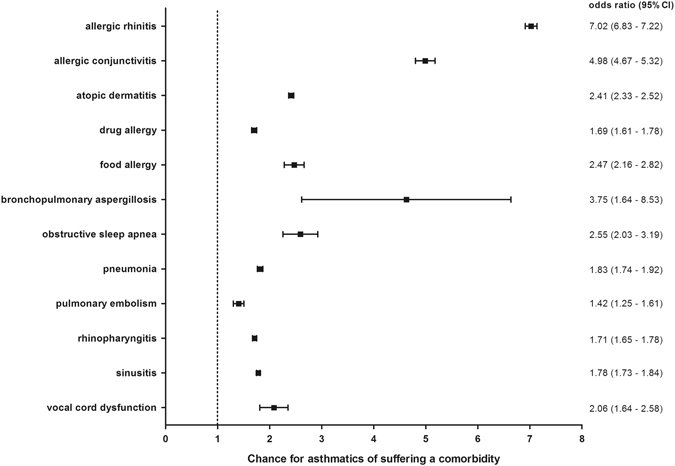
Clinical experience has shown that allergic and non-allergic respiratory, metabolic, mental, and cardiovascular disorders sometimes coexist with bronchial asthma. However, no study has been carried out that calculates the chance of manifestation of these disorders with bronchial asthma in Saarland and Rhineland-Palatinate, Germany. Using ICD10 diagnoses from health care institutions, the present study systematically analyzed the co-prevalence and odds ratios of comorbidities in the asthma population in Germany. The odds ratios were adjusted for age and sex for all comorbidities for patients with asthma vs. without asthma. Bronchial asthma was strongly associated with allergic and with a lesser extent to non-allergic comorbidities: OR 7.02 (95%CI:6.83-7.22) for allergic rhinitis; OR 4.98 (95%CI:4.67-5.32) allergic conjunctivitis; OR 2.41 (95%CI:2.33-2.52) atopic dermatitis; OR 2.47 (95%CI:2.16-2.82) food allergy, and OR 1.69 (95%CI:1.61-1.78) drug allergy. Interestingly, increased ORs were found for respiratory diseases: 2.06 (95%CI:1.64-2.58) vocal dysfunction; 1.83 (95%CI:1.74-1.92) pneumonia; 1.78 (95%CI:1.73-1.84) sinusitis; 1.71 (95%CI:1.65-1.78) rhinopharyngitis; 2.55 (95%CI:2.03-3.19) obstructive sleep apnea; 1.42 (95%CI:1.25-1.61) pulmonary embolism, and 3.75 (95%CI:1.64-8.53) bronchopulmonary aspergillosis. Asthmatics also suffer from psychiatric, metabolic, cardiac or other comorbidities. Myocardial infarction (OR 0.86, 95%CI:0.79-0.94) did not coexist with asthma. Based on the calculated chances of manifestation for these comorbidities, especially allergic and respiratory, to a lesser extent also metabolic, cardiovascular, and mental disorders should be taken into consideration in the diagnostic and treatment strategy of bronchial asthma.
PREVALENCE OF CO-EXISTING DISEASES IN GERMANY: Patients in Germany with bronchial asthma are highly likely to suffer from co-existing diseases and their treatments should reflect this. Quoc Thai Dinh at Saarland University Hospital in Homburg, Germany, and co-workers conducted a large-scale study of patients presenting with bronchial asthma in the Saarland region between 2009 and 2012. Patients with asthma made up 5.4% of the region's total population, with a higher prevalence occurring in females. They found that bronchial asthma was strongly associated with allergic comorbidities such as rhinitis. Indeed, asthmatic patients had a seven times higher chance to suffer from allergic rhinitis than the rest of the population, and were at higher risk of respiratory diseases like pneumonia and obstructive sleep apnea syndrome. Further associations included cardiovascular, metabolic and mental disorders. Dinh's team call for asthma treatments to take such comorbidities into account.
描述德国萨尔兰和莱茵兰-普法尔茨地区支气管哮喘患者合并症的流行情况,并计算其出现的机会。
利用医疗机构的 ICD10 诊断,本研究系统分析了德国哮喘人群的共病患病率和比值比。对所有共病,哮喘患者与非哮喘患者的比值比均按年龄和性别进行了调整。
支气管哮喘与过敏性共病密切相关,与非过敏性共病的相关性稍弱:过敏性鼻炎的比值比为 7.02(95%CI:6.83-7.22);过敏性结膜炎为 4.98(95%CI:4.67-5.32);特应性皮炎为 2.41(95%CI:2.33-2.52);食物过敏为 2.47(95%CI:2.16-2.82);药物过敏为 1.69(95%CI:1.61-1.78)。有趣的是,呼吸系统疾病的比值比也有所增加:发声功能障碍为 2.06(95%CI:1.64-2.58);肺炎为 1.83(95%CI:1.74-1.92);鼻窦炎为 1.78(95%CI:1.73-1.84);鼻咽炎为 1.71(95%CI:1.65-1.78);阻塞性睡眠呼吸暂停为 2.55(95%CI:2.03-3.19);肺栓塞为 1.42(95%CI:1.25-1.61);支气管肺曲霉菌病为 3.75(95%CI:1.64-8.53)。哮喘患者还患有精神、代谢、心脏或其他共病。心肌梗死(比值比 0.86,95%CI:0.79-0.94)与哮喘不共存。基于这些共病出现的概率计算,尤其是过敏性和呼吸系统疾病,在一定程度上也包括代谢、心血管和精神障碍,应在支气管哮喘的诊断和治疗策略中考虑到这些疾病。
德国患有支气管哮喘的患者极有可能同时患有其他疾病,其治疗方案应反映这一点。