Togasaki E, Takeda J, Yoshida K, Shiozawa Y, Takeuchi M, Oshima M, Saraya A, Iwama A, Yokote K, Sakaida E, Hirase C, Takeshita A, Imai K, Okumura H, Morishita Y, Usui N, Takahashi N, Fujisawa S, Shiraishi Y, Chiba K, Tanaka H, Kiyoi H, Ohnishi K, Ohtake S, Asou N, Kobayashi Y, Miyazaki Y, Miyano S, Ogawa S, Matsumura I, Nakaseko C, Naoe T
Department of Hematology, Chiba University Hospital, Chiba, Japan.
Department of Pathology and Tumor Biology, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Blood Cancer J. 2017 Apr 28;7(4):e559. doi: 10.1038/bcj.2017.36.
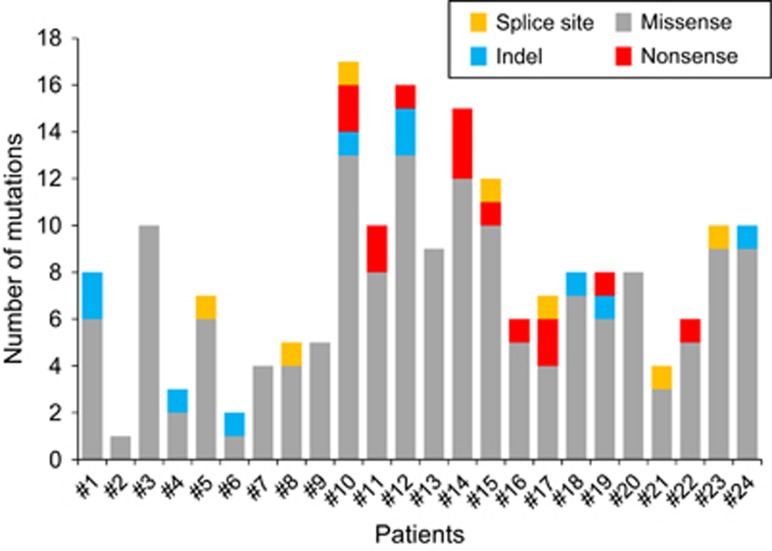
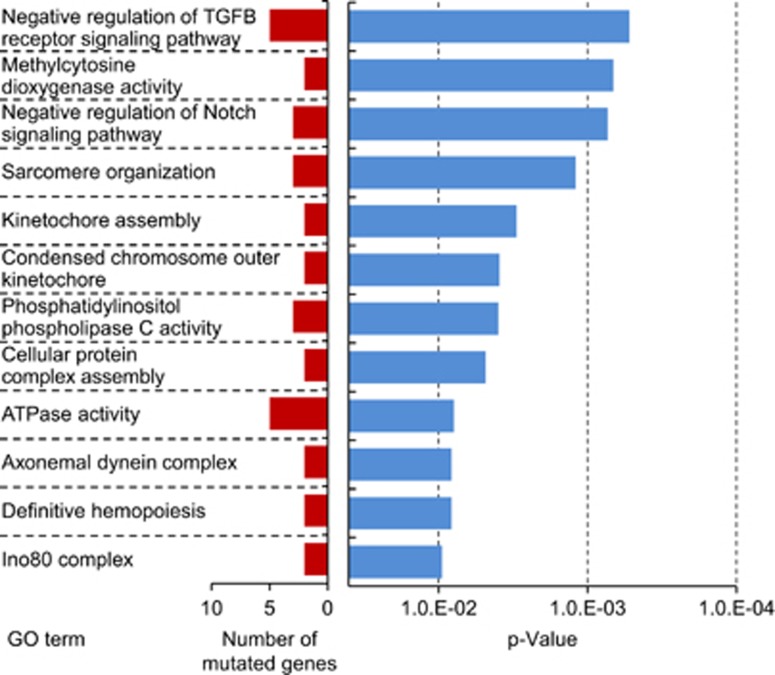
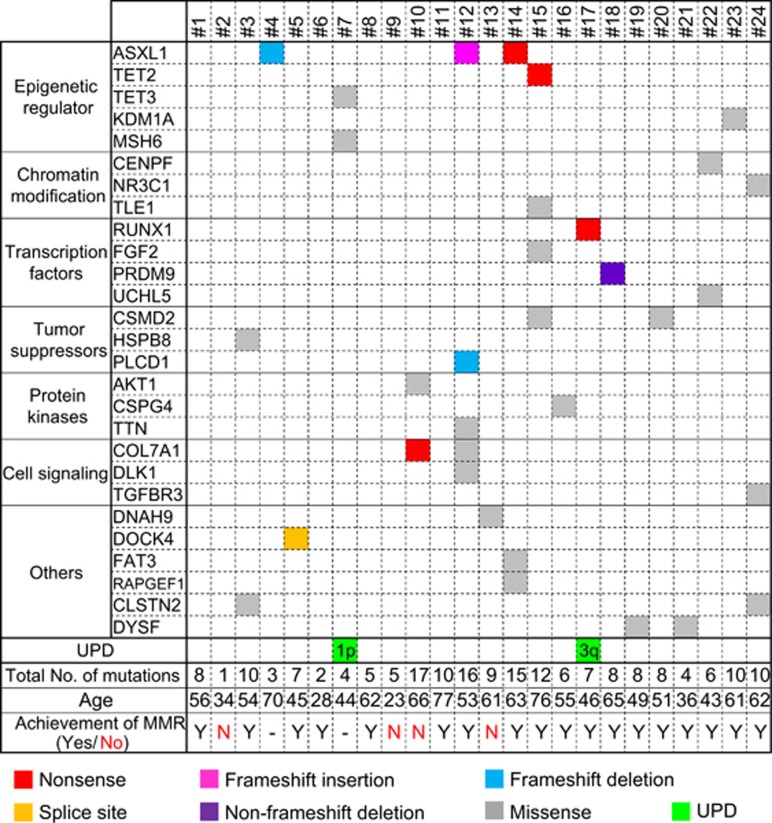
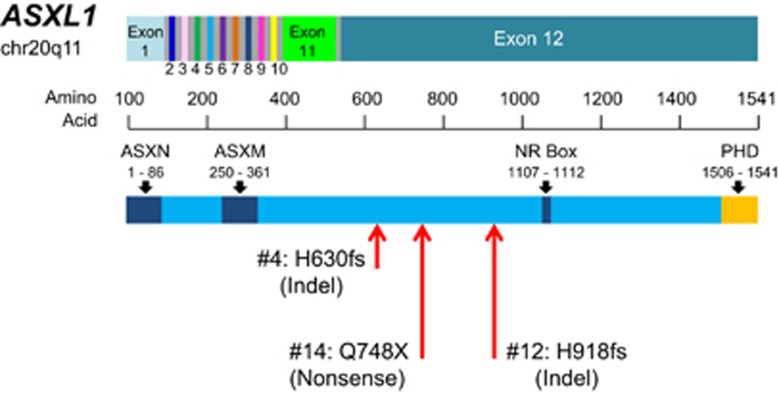
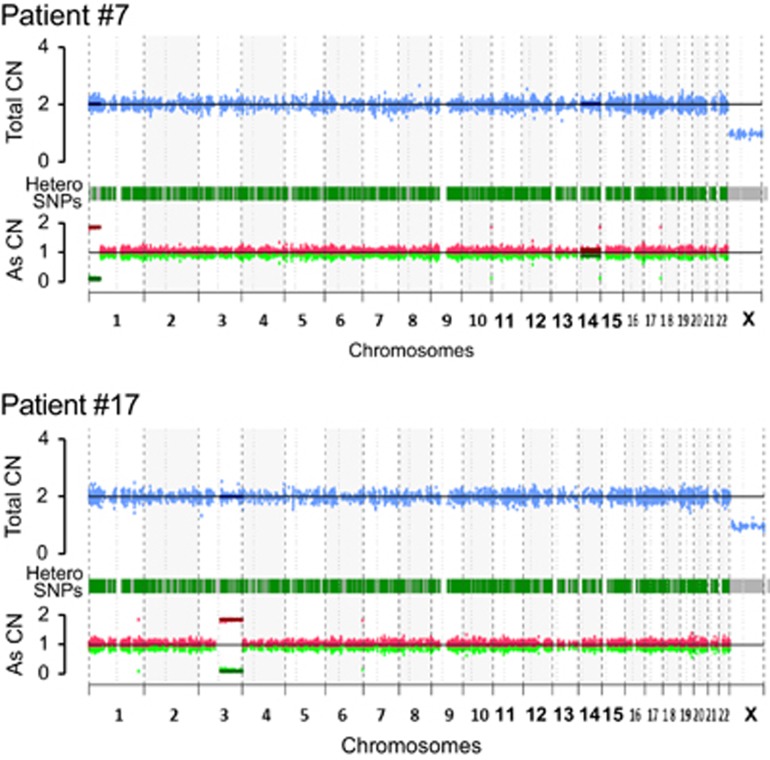
Although tyrosine kinase inhibitors (TKIs) have significantly improved the prognosis of chronic myeloid leukemia (CML), the ability of TKIs to eradicate CML remains uncertain and patients must continue TKI therapy for indefinite periods. In this study, we performed whole-exome sequencing to identify somatic mutations in 24 patients with newly diagnosed chronic phase CML who were registered in the JALSG CML212 study. We identified 191 somatic mutations other than the BCR-ABL1 fusion gene (median 8, range 1-17). Age, hemoglobin concentration and white blood cell counts were correlated with the number of mutations. Patients with mutations ⩾6 showed higher rate of achieving major molecular response than those<6 (P=0.0381). Mutations in epigenetic regulator, ASXL1, TET2, TET3, KDM1A and MSH6 were found in 25% of patients. TET2 or TET3, AKT1 and RUNX1 were mutated in one patient each. ASXL1 was mutated within exon 12 in three cases. Mutated genes were significantly enriched with cell signaling and cell division pathways. Furthermore, DNA copy number analysis showed that 2 of 24 patients had uniparental disomy of chromosome 1p or 3q, which disappeared major molecular response was achieved. These mutations may play significant roles in CML pathogenesis in addition to the strong driver mutation BCR-ABL1.
尽管酪氨酸激酶抑制剂(TKIs)显著改善了慢性髓性白血病(CML)的预后,但TKIs根除CML的能力仍不确定,患者必须无限期持续接受TKI治疗。在本研究中,我们对参加JALSG CML212研究登记的24例新诊断慢性期CML患者进行了全外显子测序,以鉴定体细胞突变。我们鉴定出191个除BCR-ABL1融合基因外的体细胞突变(中位数8个,范围1-17个)。年龄、血红蛋白浓度和白细胞计数与突变数量相关。突变数⩾6的患者达到主要分子反应的比例高于突变数<6的患者(P=0.0381)。25%的患者存在表观遗传调节因子ASXL1、TET2、TET3、KDM1A和MSH6的突变。TET2或TET3、AKT1和RUNX1各有1例患者发生突变。3例ASXL1在第12外显子内发生突变。突变基因在细胞信号传导和细胞分裂途径中显著富集。此外,DNA拷贝数分析显示,24例患者中有2例存在1号染色体p臂或3号染色体q臂单亲二体,在达到主要分子反应时消失。除了强大的驱动突变BCR-ABL1外,这些突变可能在CML发病机制中发挥重要作用。