Ferraioli Giovanna, Calcaterra Valeria, Lissandrin Raffaella, Guazzotti Marinella, Maiocchi Laura, Tinelli Carmine, De Silvestri Annalisa, Regalbuto Corrado, Pelizzo Gloria, Larizza Daniela, Filice Carlo
Ultrasound Unit, Department of Infectious Diseases, Fondazione IRCCS Policlinico San Matteo, University of Pavia, Viale Camillo Golgi 19, Pavia, 27100, Italy.
Pediatric Unit, Department of the Mother and Child Health, Fondazione IRCCS Policlinico San Matteo, University of Pavia, Pavia, Italy.
BMC Gastroenterol. 2017 May 4;17(1):61. doi: 10.1186/s12876-017-0617-6.
To assess the clinical validity of controlled attenuation parameter (CAP) in the diagnosis of hepatic steatosis in a series of overweight or obese children by using the imperfect gold standard methodology.
Consecutive children referred to our institution for auxological evaluation or obesity or minor elective surgery were prospectively enrolled. Anthropometric and biochemical parameters were recorded. Ultrasound (US) assessment of steatosis was carried out using ultrasound systems. CAP was obtained with the FibroScan 502 Touch device (Echosens, Paris, France). Pearson's or Spearman's rank correlation coefficient were used to test the association between two study variables. Optimal cutoff of CAP for detecting steatosis was 249 dB/m. The diagnostic performance of dichotomized CAP, US, body mass indexes (BMI), fatty liver index (FLI) and hepatic steatosis index (HSI) was analyzed using the imperfect gold standard methodology.
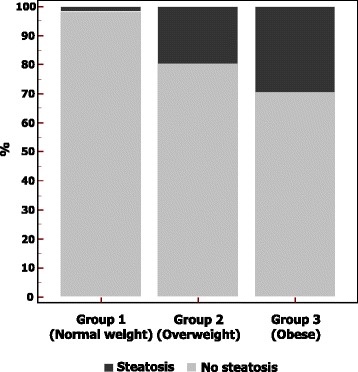
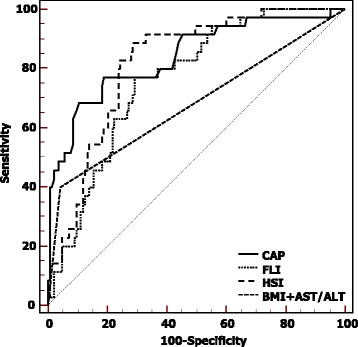
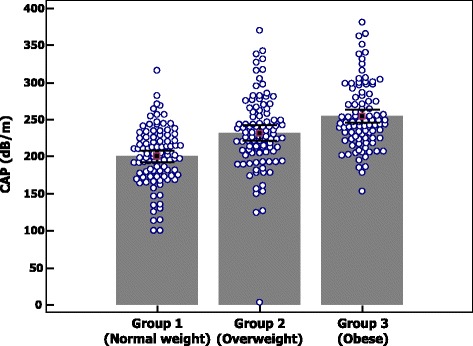
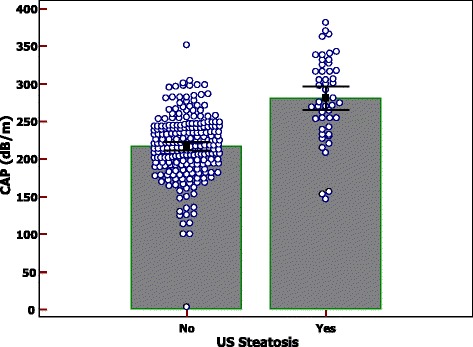
Three hundred five pediatric patients were enrolled. The data of both US and CAP were available for 289 children. Steatosis was detected in 50/289 (17.3%) children by US and in 77/289 (26.6%) by CAP. A moderate to good correlation was detected between CAP and BMI (r = 0.53), FLI (r = 0.55) and HSI (r = 0.56). In obese children a moderate to good correlation between CAP and insulin levels (r = 0.54) and HOMA-IR (r = 0.54) was also found. Dichotomized CAP showed a performance of 0.70 (sensitivity, 0.72 [0.64-0.79]; specificity, 0.98 [0.97-0.98], which was better than that of US (performance, 0.37; sensitivity, 0.46 [0.42-0.50]; specificity, 0.91 [0.89-0.92]), BMI (performance, 0.22; sensitivity, 0.75 [0.73-0.77]; specificity, 0.57 [0.55-0.60]) and FLI or HSI.
For the evaluation of liver steatosis in children CAP performs better than US, which is the most widely used imaging technique for screening patients with a suspicion of liver steatosis. A cutoff value of CAP of 249 dB/m rules in liver steatosis with a very high specificity.
采用不完善金标准方法评估受控衰减参数(CAP)在一系列超重或肥胖儿童肝脂肪变性诊断中的临床有效性。
前瞻性纳入连续转诊至我院进行生长发育评估、肥胖评估或小型择期手术的儿童。记录人体测量和生化参数。使用超声系统进行肝脂肪变性的超声(US)评估。使用FibroScan 502 Touch设备(法国巴黎Echosens公司)获取CAP。采用Pearson或Spearman等级相关系数检验两个研究变量之间的相关性。检测肝脂肪变性的CAP最佳截断值为249 dB/m。采用不完善金标准方法分析二分法CAP、US、体重指数(BMI)、脂肪肝指数(FLI)和肝脂肪变性指数(HSI)的诊断性能。
共纳入305例儿科患者。289例儿童同时获得了US和CAP数据。US检测到50/289例(17.3%)儿童存在肝脂肪变性,CAP检测到77/289例(26.6%)。CAP与BMI(r = 0.53)、FLI(r = 0.55)和HSI(r = 0.56)之间存在中度至良好的相关性。在肥胖儿童中,还发现CAP与胰岛素水平(r = 0.54)和HOMA-IR(r = 0.54)之间存在中度至良好的相关性。二分法CAP的诊断性能为0.70(敏感性,0.72[0.64 - 0.79];特异性,0.98[0.97 - 0.98]),优于US(诊断性能,0.37;敏感性,0.46[0.42 - 0.50];特异性,0.91[0.89 - 0.92])、BMI(诊断性能,0.22;敏感性,0.75[0.73 - 0.77];特异性,0.57[0.55 - 0.60])以及FLI或HSI。
对于儿童肝脂肪变性的评估,CAP的表现优于US,US是目前用于筛查疑似肝脂肪变性患者最广泛使用的成像技术。CAP截断值为249 dB/m时,诊断肝脂肪变性具有非常高的特异性。