de Fine Licht Sofie, Rugbjerg Kathrine, Gudmundsdottir Thorgerdur, Bonnesen Trine G, Asdahl Peter Haubjerg, Holmqvist Anna Sällfors, Madanat-Harjuoja Laura, Tryggvadottir Laufey, Wesenberg Finn, Hasle Henrik, Winther Jeanette F, Olsen Jørgen H
Danish Cancer Society Research Center, Copenhagen, Denmark.
Department of Paediatrics, Aarhus University Hospital, Aarhus, Denmark.
PLoS Med. 2017 May 9;14(5):e1002296. doi: 10.1371/journal.pmed.1002296. eCollection 2017 May.
Survivors of childhood cancer are at increased risk for a wide range of late effects. However, no large population-based studies have included the whole range of somatic diagnoses including subgroup diagnoses and all main types of childhood cancers. Therefore, we aimed to provide the most detailed overview of the long-term risk of hospitalisation in survivors of childhood cancer.
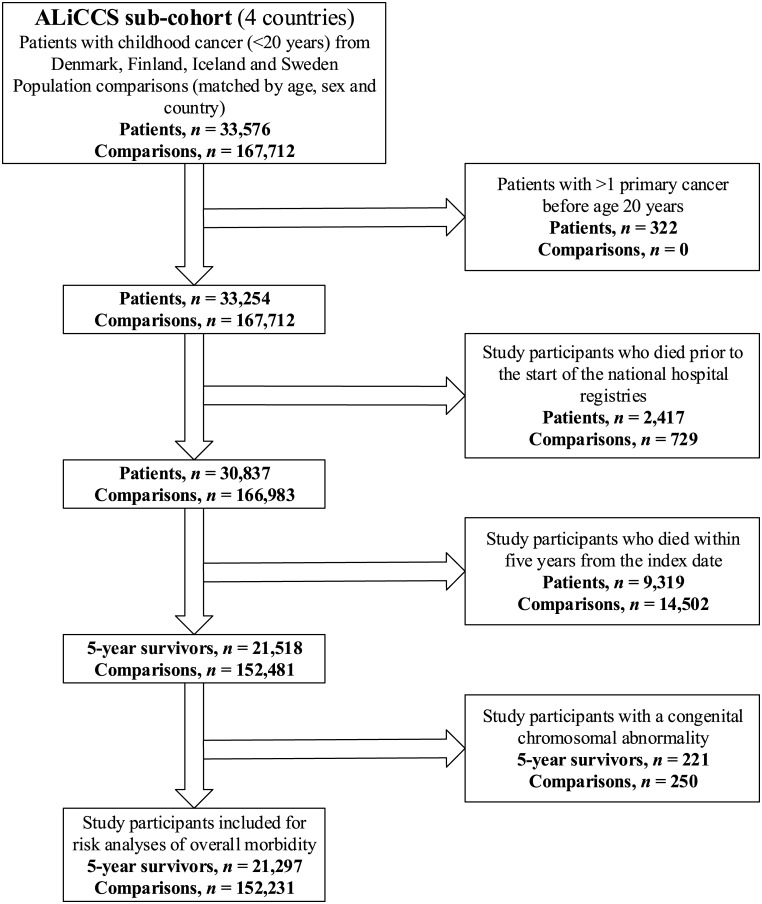
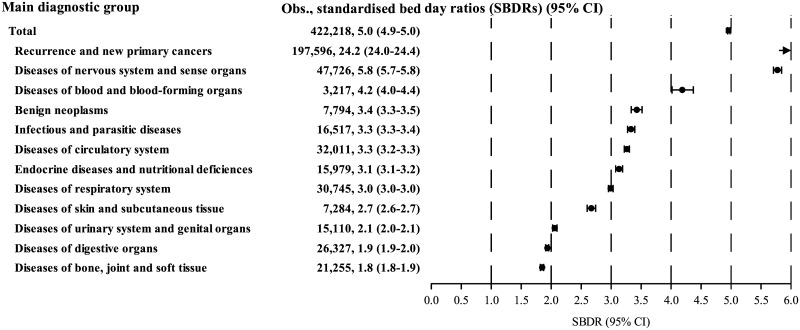
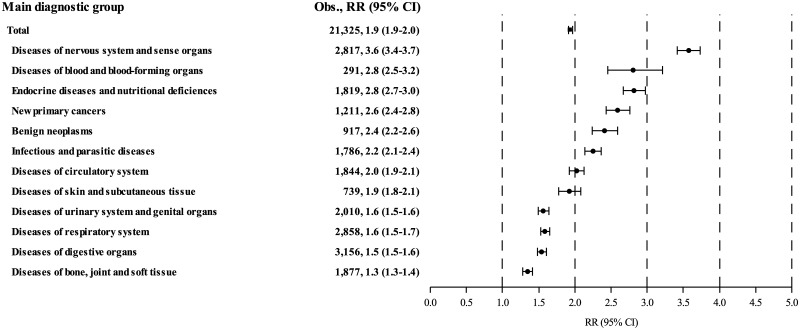
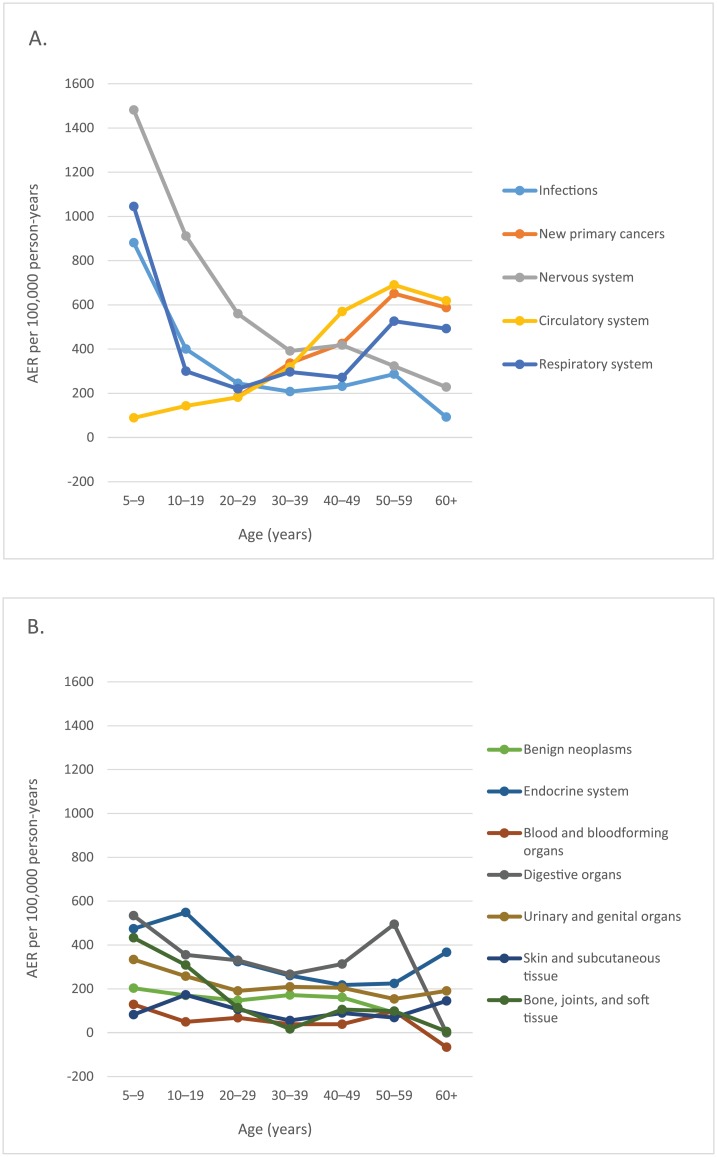
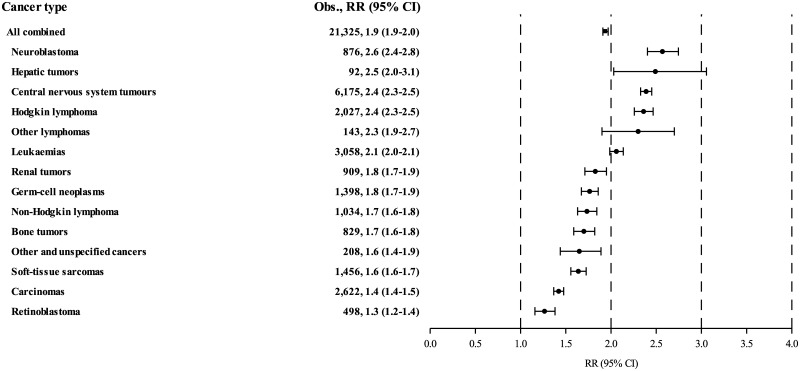
From the national cancer registers of Denmark, Finland, Iceland, and Sweden, we identified 21,297 5-year survivors of childhood cancer diagnosed with cancer before the age of 20 years in the periods 1943-2008 in Denmark, 1971-2008 in Finland, 1955-2008 in Iceland, and 1958-2008 in Sweden. We randomly selected 152,231 population comparison individuals matched by age, sex, year, and country (or municipality in Sweden) from the national population registers. Using a cohort design, study participants were followed in the national hospital registers in Denmark, 1977-2010; Finland, 1975-2012; Iceland, 1999-2008; and Sweden, 1968-2009. Disease-specific hospitalisation rates in survivors and comparison individuals were used to calculate survivors' standardised hospitalisation rate ratios (RRs), absolute excess risks (AERs), and standardised bed day ratios (SBDRs) based on length of stay in hospital. We adjusted for sex, age, and year by indirect standardisation. During 336,554 person-years of follow-up (mean: 16 years; range: 0-42 years), childhood cancer survivors experienced 21,325 first hospitalisations for diseases in one or more of 120 disease categories (cancer recurrence not included), when 10,999 were expected, yielding an overall RR of 1.94 (95% confidence interval [95% CI] 1.91-1.97). The AER was 3,068 (2,980-3,156) per 100,000 person-years, meaning that for each additional year of follow-up, an average of 3 of 100 survivors were hospitalised for a new excess disease beyond the background rates. Approximately 50% of the excess hospitalisations were for diseases of the nervous system (19.1% of all excess hospitalisations), endocrine system (11.1%), digestive organs (10.5%), and respiratory system (10.0%). Survivors of all types of childhood cancer were at increased, persistent risk for subsequent hospitalisation, the highest risks being those of survivors of neuroblastoma (RR: 2.6 [2.4-2.8]; n = 876), hepatic tumours (RR: 2.5 [2.0-3.1]; n = 92), central nervous system tumours (RR: 2.4 [2.3-2.5]; n = 6,175), and Hodgkin lymphoma (RR: 2.4 [2.3-2.5]; n = 2,027). Survivors spent on average five times as many days in hospital as comparison individuals (SBDR: 4.96 [4.94-4.98]; n = 422,218). The analyses of bed days in hospital included new primary cancers and recurrences. Of the total 422,218 days survivors spent in hospital, 47% (197,596 bed days) were for new primary cancers and recurrences. Our study is likely to underestimate the absolute overall disease burden experienced by survivors, as less severe late effects are missed if they are treated sufficiently in the outpatient setting or in the primary health care system.
Childhood cancer survivors were at increased long-term risk for diseases requiring inpatient treatment even decades after their initial cancer. Health care providers who do not work in the area of late effects, especially those in primary health care, should be aware of this highly challenged group of patients in order to avoid or postpone hospitalisations by prevention, early detection, and appropriate treatments.
儿童癌症幸存者面临多种晚期效应的风险增加。然而,尚无大型基于人群的研究涵盖所有躯体诊断类型,包括亚组诊断以及所有主要类型的儿童癌症。因此,我们旨在提供儿童癌症幸存者住院长期风险的最详细概述。
我们从丹麦、芬兰、冰岛和瑞典的国家癌症登记处,识别出1943 - 2008年丹麦、1971 - 2008年芬兰、1955 - 2008年冰岛以及1958 - 2008年瑞典中21,297名20岁前被诊断为儿童癌症的5年幸存者。我们从国家人口登记处随机选取了152,231名按年龄、性别、年份和国家(瑞典为直辖市)匹配的人群作为对照个体。采用队列设计,在丹麦(1977 - 2010年)、芬兰(1975 - 2012年)、冰岛(1999 - 2008年)和瑞典(1968 - 2009年)的国家医院登记处对研究参与者进行随访。根据幸存者和对照个体的疾病特异性住院率,基于住院时长计算幸存者的标准化住院率比(RRs)、绝对超额风险(AERs)和标准化床日比(SBDRs)。我们通过间接标准化对性别、年龄和年份进行了调整。在336,554人年的随访期间(平均:16年;范围:0 - 42年),儿童癌症幸存者因120种疾病类别中的一种或多种疾病首次住院21,325次(不包括癌症复发),而预期为10,999次,总体RR为1.94(95%置信区间[95%CI]1.91 - 1.97)。AER为每100,000人年3,068(2,980 - 3,156),这意味着每增加一年的随访,每100名幸存者中平均有3人因超出背景发病率的新的额外疾病住院。约50%的额外住院是因神经系统疾病(占所有额外住院的19.1%)、内分泌系统疾病(11.1%)、消化器官疾病(10.5%)和呼吸系统疾病(10.0%)。所有类型儿童癌症的幸存者后续住院风险均增加且持续存在,风险最高的是神经母细胞瘤幸存者(RR:2.6[2.4 - 2.8];n = 876)、肝肿瘤幸存者(RR:2.5[2.0 - 3.1];n = 92)、中枢神经系统肿瘤幸存者(RR:2.4[2.3 - 2.5];n = 6,175)和霍奇金淋巴瘤幸存者(RR:2.4[2.3 - 2.5];n = 2,027)。幸存者平均住院天数是对照个体的五倍(SBDR:4.96[4.94 - 4.98];n = 422,218)。住院床日分析包括新发原发性癌症和复发。在幸存者住院的422,218天中,47%(197,596个床日)是因新发原发性癌症和复发。我们的研究可能低估了幸存者所经历的绝对总体疾病负担,因为如果较轻的晚期效应在门诊或初级卫生保健系统中得到充分治疗,可能会被遗漏。
即使在初次患癌数十年后,儿童癌症幸存者因需要住院治疗的疾病而面临的长期风险仍会增加。不在晚期效应领域工作的医疗保健提供者,尤其是初级卫生保健领域的提供者,应了解这一极具挑战性的患者群体,以便通过预防、早期检测和适当治疗避免或推迟住院治疗。