Ong Charlene Jennifer, Gluckstein Jeffrey, Laurido-Soto Osvaldo, Yan Yan, Dhar Rajat, Lee Jin-Moo
From the Department of Neurology, Massachusetts General Hospital/Brigham and Women's Hospital/Harvard Medical School, Boston (C.J.O., J.G.); and Department of Neurology, Washington University School of Medicine, St. Louis, MO (O.L.-S., Y.Y., R.D., J.-M.L.).
Stroke. 2017 Jul;48(7):1969-1972. doi: 10.1161/STROKEAHA.117.016733. Epub 2017 May 9.
Rapid recognition of those at high risk for malignant edema after stroke would facilitate triage for monitoring and potential surgery. Admission data may be insufficient for accurate triage decisions. We developed a risk prediction score using clinical and radiographic variables within 24 hours of ictus to better predict potentially lethal malignant edema.
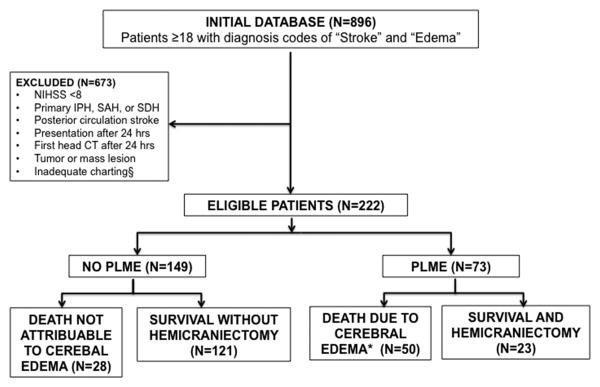
Patients admitted with diagnosis codes of cerebral edema and ischemic stroke, NIHSS score (National Institute of Health Stroke Score) of ≥8 and head computed tomographies within 24 hours of stroke onset were included. Primary outcome of potentially lethal malignant edema was defined as death with midline shift ≥5 mm or decompressive hemicraniectomy. We performed multivariate analyses on data available within 24 hours of ictus. Bootstrapping was used to internally validate the model, and a risk score was constructed from the results.
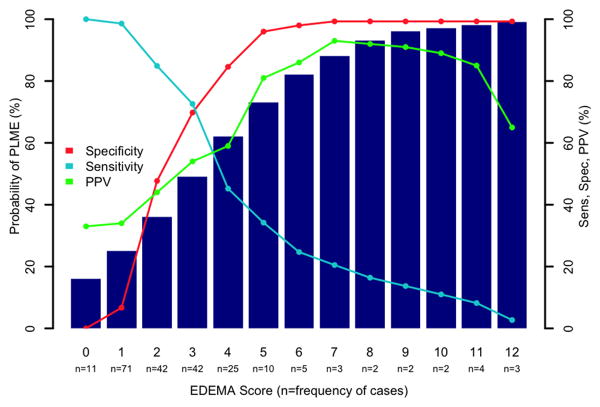
Thirty-three percent of 222 patients developed potentially lethal malignant edema. The final model C statistic was 0.76 (confidence interval, 0.68-0.82) in the derivation cohort and 0.75 (confidence interval, 0.72-0.77) in the bootstrapping validation sample. The EDEMA score (Enhanced Detection of Edema in Malignant Anterior Circulation Stroke) was developed using the following independent predictors: basal cistern effacement (=3); glucose ≥150 (=2); no tPA (tissue-type plasminogen activator) or thrombectomy (=1), midline shift >0 to 3 (=1), 3 to 6 (=2), and 6 to 9 (=4); >9 (=7); and no previous stroke (=1). A score over 7 was associated with 93% positive predictive value.
The EDEMA score identifies patients at high risk for potentially lethal malignant edema. Although it requires external validation, this scale could help expedite triage decisions in this patient population.
快速识别卒中后发生恶性水肿的高危患者将有助于进行分诊以进行监测和可能的手术治疗。入院数据可能不足以做出准确的分诊决策。我们利用发病24小时内的临床和影像学变量制定了一个风险预测评分,以更好地预测潜在致命性恶性水肿。
纳入诊断编码为脑水肿和缺血性卒中、美国国立卫生研究院卒中量表(NIHSS)评分≥8且在卒中发病24小时内进行头颅计算机断层扫描的患者。潜在致命性恶性水肿的主要结局定义为伴有中线移位≥5mm的死亡或去骨瓣减压术。我们对发病24小时内可获得的数据进行多变量分析。采用自抽样法对模型进行内部验证,并根据结果构建风险评分。
222例患者中有33%发生了潜在致命性恶性水肿。推导队列中最终模型的C统计量为0.76(置信区间为0.68 - 0.82),自抽样验证样本中为0.75(置信区间为0.72 - 0.77)。利用以下独立预测因素制定了EDEMA评分(恶性前循环卒中水肿增强检测评分):基底池消失(=3);血糖≥150(=2);未使用组织型纤溶酶原激活剂(tPA)或未行血栓切除术(=1),中线移位>0至3(=1)、3至6(=2)以及6至9(=4);>9(=7);既往无卒中(=1)。评分超过7与93%的阳性预测值相关。
EDEMA评分可识别潜在致命性恶性水肿的高危患者。尽管它需要外部验证,但该量表有助于加快对这类患者的分诊决策。