Centre for Experimental Medicine and Rheumatology, William Harvey Research Institute, Barts and the London School of Medicine and Dentistry, Queen Mary University of London, Charterhouse Square, London, EC1M 6BQ, UK.
Kennedy Institute of Rheumatology, Oxford University, Oxford, UK.
Clin Rev Allergy Immunol. 2017 Oct;53(2):265-276. doi: 10.1007/s12016-017-8610-y.
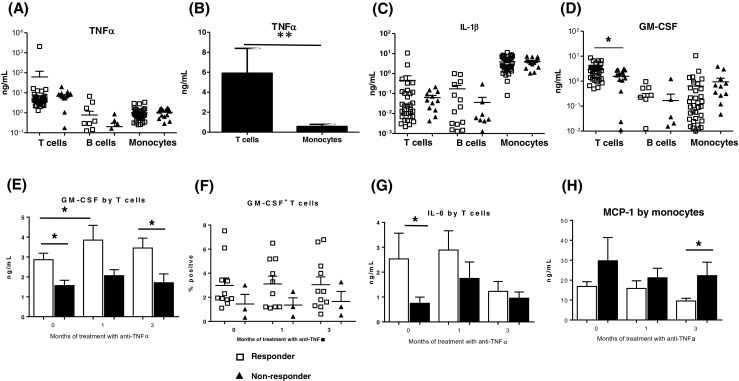
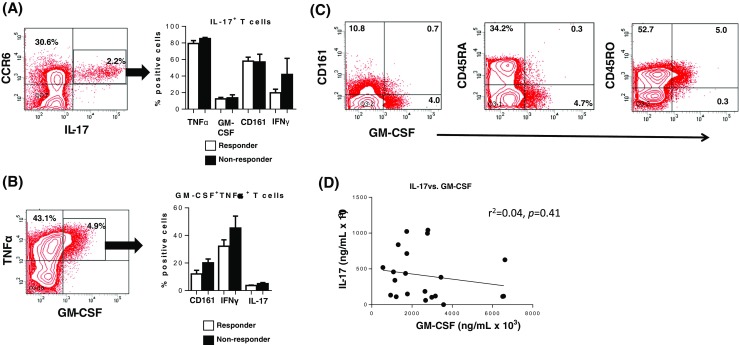
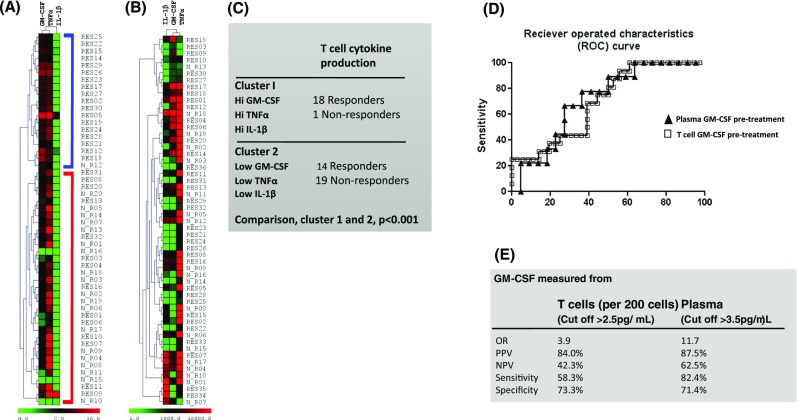
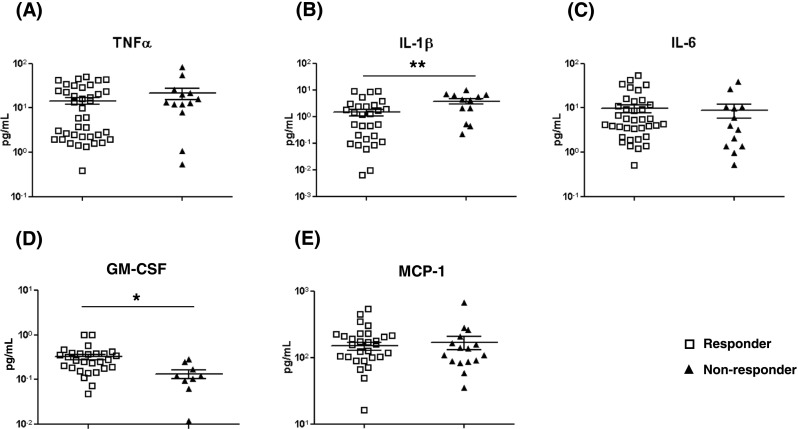
Biologic TNFα inhibitors are a mainstay treatment option for patients with rheumatoid arthritis (RA) refractory to other treatment options. However, many patients either do not respond or relapse after initially responding to these agents. This study was carried out to identify biomarkers that can distinguish responder from non-responder patients before the initiation of treatment. The level of cytokines in plasma and those produced by ex vivo T cells, B cells and monocytes in 97 RA patients treated with biologic TNFα inhibitors was measured before treatment and after 1 and 3 months of treatment by multiplex analyses. The frequency of T cell subsets and intracellular cytokines were determined by flow cytometry. The results reveal that pre-treatment, T cells from patients who went on to respond to treatment with biologic anti-TNFα agents produced significantly more GM-CSF than non-responder patients. Furthermore, immune cells from responder patients produced higher levels of IL-1β, TNFα and IL-6. Cytokine profiling in the blood of patients confirmed the association between high levels of GM-CSF and responsiveness to biologic anti-TNFα agents. Thus, high blood levels of GM-CSF pre-treatment had a positive predictive value of 87.5% (61.6 to 98.5% at 95% CI) in treated RA patients. The study also shows that cells from most anti-TNFα responder patients in the current cohort produced higher levels of GM-CSF and TNFα pre-treatment than non-responder patients. Findings from the current study and our previous observations that non-responsiveness to anti-TNFα is associated with high IL-17 levels suggest that the disease in responder and non-responder RA patients is likely to be driven/sustained by different inflammatory pathways. The use of biomarker signatures of distinct pro-inflammatory pathways could lead to evidence-based prescription of the most appropriate biological therapies for different RA patients.
生物制剂 TNFα 抑制剂是治疗类风湿关节炎(RA)患者的主要选择,这些患者对其他治疗方法无反应或初始治疗后复发。本研究旨在确定生物制剂 TNFα 抑制剂治疗前可区分应答者和无应答者的生物标志物。通过多重分析,在 97 例接受生物制剂 TNFα 抑制剂治疗的 RA 患者治疗前、治疗 1 个月和 3 个月时测量了其血浆细胞因子水平和体外 T 细胞、B 细胞和单核细胞产生的细胞因子水平。通过流式细胞术测定 T 细胞亚群和细胞内细胞因子的频率。结果表明,与无应答者相比,治疗后应答者治疗前 T 细胞产生的 GM-CSF 明显更多。此外,应答者免疫细胞产生的 IL-1β、TNFα 和 IL-6 水平更高。患者血液中的细胞因子谱证实了 GM-CSF 水平与对生物制剂抗 TNFα 药物的反应之间存在关联。因此,治疗 RA 患者中 GM-CSF 治疗前血液水平具有 87.5%的阳性预测值(95%CI 为 61.6%至 98.5%)。该研究还表明,当前队列中大多数对 TNFα 应答的患者的细胞在治疗前产生的 GM-CSF 和 TNFα 水平高于无应答者。本研究和我们之前的观察结果表明,对 TNFα 的无反应与高 IL-17 水平有关,这表明应答者和无应答者 RA 患者的疾病可能由不同的炎症途径驱动/维持。使用不同促炎途径的生物标志物特征可能会导致针对不同 RA 患者的最适当生物治疗的基于证据的处方。