Botnar Research Centre, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Windmill Road, Oxford, OX3 7LD, UK.
Takeda Development Centre, London, UK.
Arthritis Res Ther. 2019 Apr 18;21(1):101. doi: 10.1186/s13075-019-1879-x.
Namilumab (AMG203), an immunoglobulin G1 monoclonal antibody that binds with high affinity to granulocyte-macrophage colony-stimulating factor (GM-CSF), was evaluated in a phase II randomized, double-blind, placebo-controlled study to investigate the efficacy and safety in patients with rheumatoid arthritis (RA) with an inadequate response to methotrexate (MTX-IR) or anti-tumour necrosis factor therapy (TNF-IR).
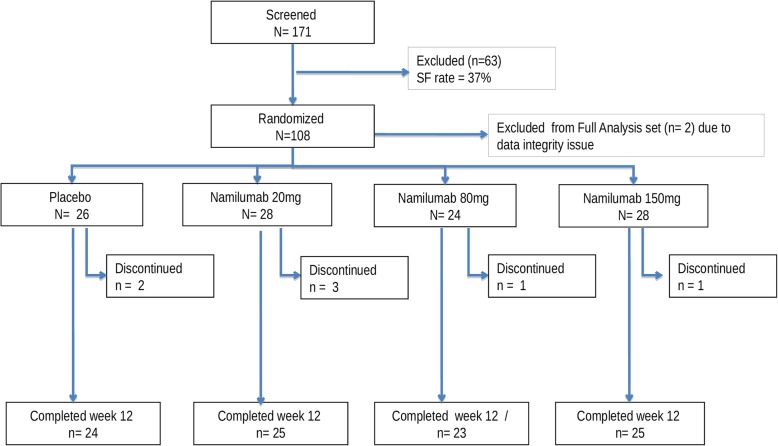
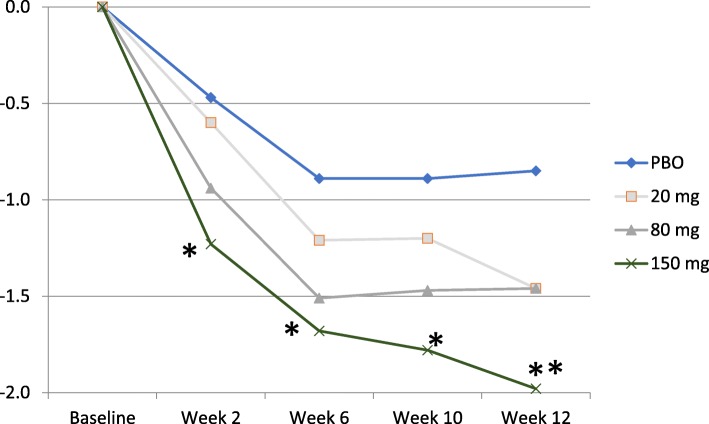
Subcutaneous namilumab (20, 80, or 150 mg) or placebo was administered at baseline and weeks 2, 6, and 10 in patients on stable background methotrexate therapy who were with MTX-IR or TNF-IR. Primary endpoint was mean change from baseline in the 28-joint Disease Activity Score, C-reactive protein version (DAS28-CRP) at week 12 comparing each of the three doses of namilumab to placebo. Safety and tolerability were assessed by adverse events (AEs) and pulmonary parameters. Results were analysed using the per-protocol population.
One hundred eight patients from Europe and Japan (48.4 ± 12.02 years old; 77.8% female; mean DAS28-CRP 5.60-5.79; rheumatoid factor/anti-citrullinated protein antibodies + 75%) were randomized to placebo or namilumab 20, 80, or 150 mg (n = 27, 28, 25, and 28, respectively). Ninety-two were MTX-IR; 16 were TNF-IR. At week 12, a statistically significant difference in DAS28-CRP (p = 0.005) was seen for namilumab 150 mg versus placebo and separation was seen as early as week 2 for namilumab 150 mg (p < 0.05), with higher ACR50 and response rates versus placebo at week 12. A dose-response effect was observed across the DAS28-CRP endpoint with separation versus placebo evident from week 2. The most common treatment-emergent AEs were nasopharyngitis (18.5%, 17.9%, 4.0%, 14.3%), dyspnoea (0.0%, 3.6%, 8.0%, 10.7%), bronchitis (7.4%, 3.6%, 4.0%, 3.6%), and headache (3.7%, 3.6%, 12.0%, 0.0%) for placebo and 20, 80, or 150 mg of namilumab, respectively. No serious infections were observed. One serious AE (myocardial infarction) was observed with 150 mg of namilumab. There was no apparent dose relationship for AEs. A biomarker-based disease activity score showed a dose-dependent decrease at week 12.
This phase II study demonstrates the benefit of inhibiting macrophage activity targeting the GM-CSF for RA. The study met its primary endpoint with a clear dose-response effect. An acceptable tolerability profile was demonstrated over the 12-week study.
ClinicalTrials.gov, NEXUS; NCT02379091 , submitted November 28, 2014.
纳武利尤单抗(AMG203)是一种高亲和力结合粒细胞-巨噬细胞集落刺激因子(GM-CSF)的免疫球蛋白 G1 单克隆抗体,在一项 II 期随机、双盲、安慰剂对照研究中进行了评估,以研究对甲氨蝶呤(MTX-IR)或抗肿瘤坏死因子治疗(TNF-IR)反应不足的类风湿关节炎(RA)患者的疗效和安全性。
在稳定接受甲氨蝶呤治疗的患者中,皮下给予纳武利尤单抗(20、80 或 150mg)或安慰剂,基线时和第 2、6 和 10 周给药,这些患者对 MTX-IR 或 TNF-IR 反应不足。主要终点是比较每组三种剂量的纳武利尤单抗与安慰剂在第 12 周时 28 关节疾病活动评分(DAS28-CRP)的平均变化。安全性和耐受性通过不良事件(AE)和肺参数评估。使用方案人群进行分析。
来自欧洲和日本的 108 名患者(48.4±12.02 岁;77.8%女性;平均 DAS28-CRP 5.60-5.79;类风湿因子/抗瓜氨酸蛋白抗体阳性+75%)被随机分配至安慰剂或纳武利尤单抗 20、80 或 150mg 组(n=27、28、25 和 28)。92 名患者对 MTX-IR;16 名患者对 TNF-IR。在第 12 周,纳武利尤单抗 150mg 与安慰剂相比 DAS28-CRP 有统计学意义的差异(p=0.005),纳武利尤单抗 150mg 早在第 2 周就出现了分离(p<0.05),并且在第 12 周时与安慰剂相比 ACR50 和反应率更高。在 DAS28-CRP 终点上观察到剂量反应效应,从第 2 周开始与安慰剂分离。最常见的治疗相关不良事件是鼻咽炎(18.5%、17.9%、4.0%、14.3%)、呼吸困难(0.0%、3.6%、8.0%、10.7%)、支气管炎(7.4%、3.6%、4.0%、3.6%)和头痛(3.7%、3.6%、12.0%、0.0%),分别对应安慰剂和 20、80 或 150mg 的纳武利尤单抗。未观察到严重感染。纳武利尤单抗 150mg 组发生 1 例严重不良事件(心肌梗死)。AE 与剂量之间似乎没有明显的关系。基于生物标志物的疾病活动评分显示在第 12 周时呈剂量依赖性下降。
这项 II 期研究证明了针对 RA 抑制巨噬细胞活性靶向 GM-CSF 的益处。该研究达到了主要终点,具有明显的剂量反应效应。在 12 周的研究中表现出可接受的耐受性。
ClinicalTrials.gov,NEXUS;NCT02379091,于 2014 年 11 月 28 日提交。