Gemmell L C, Webster K E, Kirtley S, Vincent K, Zondervan K T, Becker C M
Case Western Reserve School of Medicine, 10900 Euclid Avenue, Cleveland, OH 44106, USA.
Endometriosis CaRe Centre, Nuffield Department of Obstetrics and Gynaecology, University of Oxford, John Radcliffe Hospital, Women's Centre, Oxford OX3 9DU, UK.
Hum Reprod Update. 2017 Jul 1;23(4):481-500. doi: 10.1093/humupd/dmx011.
Endometriosis is typically regarded as a premenopausal disease, resolving after natural or iatrogenic menopause due to declining oestrogen levels. Nonetheless, case reports over the years have highlighted the incidence of recurrent postmenopausal endometriosis. It is now clear that both recurrence and malignant transformation of endometriotic foci can occur in the postmenopausal period. Postmenopausal women are commonly treated with hormone replacement therapy (HRT) to treat climacteric symptoms and prevent bone loss; however, HRT may reactivate endometriosis and stimulate malignant transformation in women with a history of endometriosis. Given the uncertain risks of initiating HRT, it is difficult to determine the best menopausal management for this group of women.
The aim of this study was to systematically review the existing literature on management of menopausal symptoms in women with a history of endometriosis. We also aimed to evaluate the published literature on the risks associated with HRT in these women, and details regarding optimal formulations and timing (i.e. initiation and duration) of HRT.
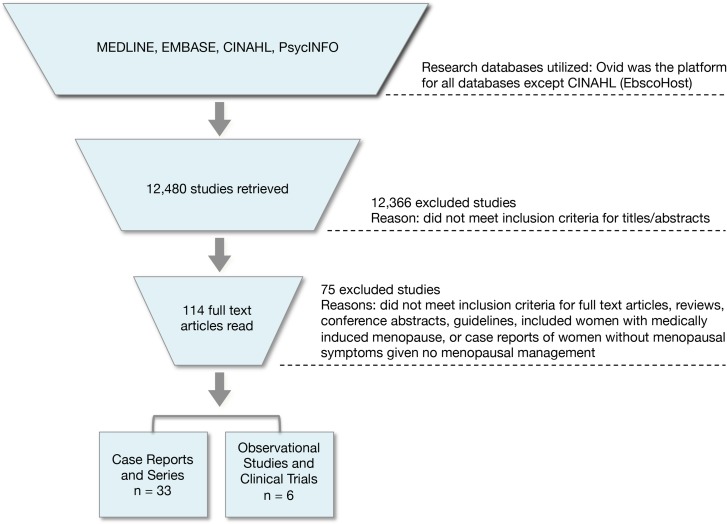
Four electronic databases (MEDLINE via OVID, Embase via OVID, PsycINFO via OVID and CINAHL via EbscoHost) were searched from database inception until June 2016, using a combination of relevant controlled vocabulary terms and free-text terms related to 'menopause' and 'endometriosis'. Inclusion criteria were: menopausal women with a history of endometriosis and menopausal treatment including HRT or other preparations. Case reports/series, observational studies and clinical trials were included. Narrative review articles, organizational guidelines and conference abstracts were excluded, as were studies that did not report on any form of menopausal management. Articles were assessed for risk of bias and quality using GRADE criteria.
We present a synthesis of the existing case reports of endometriosis recurrence or malignant transformation in women undergoing treatment for menopausal symptoms. We highlight common presenting symptoms, potential risk factors and outcomes amongst the studies. Sparse high-quality evidence was identified, with few observational studies and only two randomized controlled trials. Given this paucity of data, no definitive conclusions can be drawn concerning risk.
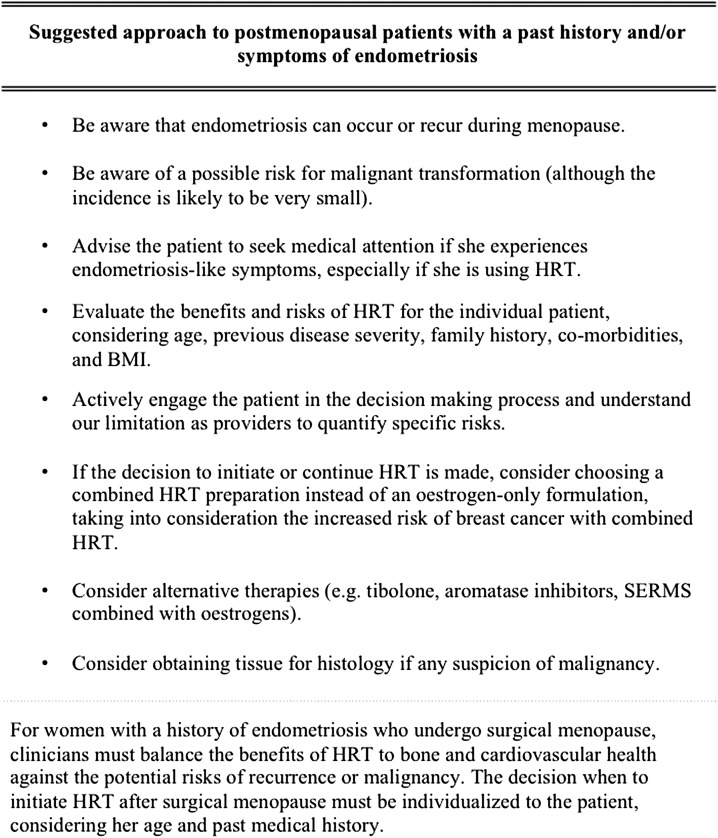
Due to the lack of high-quality studies, it remains unclear how to advise women with a history of endometriosis regarding the management of menopausal symptoms. The absolute risk of disease recurrence and malignant transformation cannot be quantified, and the impact of HRT use on these outcomes is not known. Multicentre randomized trials or large observational studies are urgently needed to inform clinicians and patients alike.
子宫内膜异位症通常被视为一种绝经前疾病,由于雌激素水平下降,在自然绝经或医源性绝经后会自行缓解。尽管如此,多年来的病例报告凸显了绝经后复发性子宫内膜异位症的发生率。现在很清楚,子宫内膜异位病灶的复发和恶性转化在绝经后时期均可能发生。绝经后女性通常接受激素替代疗法(HRT)来治疗更年期症状并预防骨质流失;然而,HRT可能会使有子宫内膜异位症病史的女性的子宫内膜异位症重新激活并刺激恶性转化。鉴于启动HRT存在不确定的风险,很难为这组女性确定最佳的绝经管理方案。
本研究的目的是系统回顾有关有子宫内膜异位症病史女性更年期症状管理的现有文献。我们还旨在评估已发表的关于这些女性中与HRT相关风险的文献,以及关于HRT的最佳配方和时机(即开始时间和持续时间)的详细信息。
从数据库建立至2016年6月,使用与“绝经”和“子宫内膜异位症”相关的相关控制词汇和自由文本词的组合,对四个电子数据库(通过OVID的MEDLINE、通过OVID的Embase、通过OVID的PsycINFO和通过EbscoHost的CINAHL)进行检索。纳入标准为:有子宫内膜异位症病史的绝经女性以及包括HRT或其他制剂的绝经治疗。纳入病例报告/系列、观察性研究和临床试验。排除叙述性综述文章、组织指南和会议摘要,以及未报告任何形式绝经管理的研究。使用GRADE标准评估文章的偏倚风险和质量。
我们对接受更年期症状治疗的女性中子宫内膜异位症复发或恶性转化的现有病例报告进行了综合分析。我们强调了这些研究中的常见症状、潜在危险因素和结果。发现高质量证据稀少,观察性研究很少,只有两项随机对照试验。鉴于数据匮乏,无法就风险得出明确结论。
由于缺乏高质量研究,目前尚不清楚如何就更年期症状的管理向有子宫内膜异位症病史的女性提供建议。疾病复发和恶性转化的绝对风险无法量化,HRT使用对这些结果的影响也未知。迫切需要多中心随机试验或大型观察性研究,为临床医生和患者提供信息。