Department of Cardiology, Hospital General Universitario Gregorio Marañón, Doctor Esquerdo 46, 28007, Madrid, Spain.
Department of Palliative Care, Hospital General Universitario Gregorio Marañón, Madrid, Spain.
BMC Palliat Care. 2017 May 22;16(1):35. doi: 10.1186/s12904-017-0208-x.
Dyspnoea is a disabling symptom in patients admitted with heart failure (HF) and respiratory diseases (RD). The main aim of this study is to evaluate its intensity at admission and discharge and the relation with quality of life. We also describe its management, intensity, and evolution in HF and RD.
In this descriptive, cross-sectional study, we included prospectively all patients admitted with decompensated HF and chronic obstructive pulmonary disease (COPD)/pulmonary fibrosis during 4 months. Surveys quantifying dyspnoea (Numerical Rating Scale 1-10) and quality of life (EuroQoL 5d) were administered at discharge.
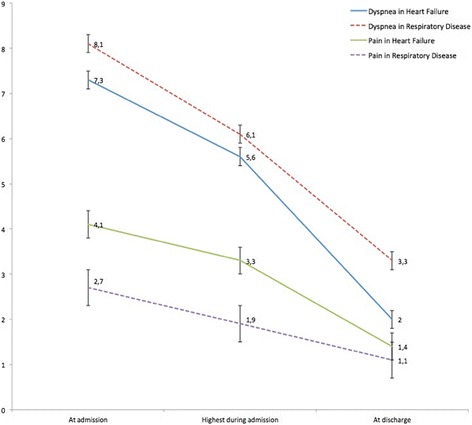
A total of 258 patients were included: 190 (73.6%) with HF and 68 (26.4%) with RD (62 COPD and 6 pulmonary fibrosis). Mean age was 74.0±1.2 years, and 157 (60.6%) were men. Dyspnoea before admission was 7.5±0.1. Patients with RD showed greater dyspnoea than those with HF both before admission (8.1±0.2 vs. 7.3±0.2, p=0.01) and at discharge (3.2±0.3 vs. 2.0±0.2, p=0.0001). They also presented a higher rate of severe dyspnoea (≥5) at discharge (23 [34.3%] vs. 36 [19.1%], p=0.02). Opioids were used in 41 (15.9%), mean dose 8.7±0.8 mg Morphine Equivalent Daily Dose. HF patients had worse EuroQoL 5d scores than those with RD, due to mobility problems (118 [62.1%] vs. 28 [41.8%], p=0.004), and lower punctuation in Visual Analogue Scale (57.9±1.6 vs. 65.6±1.0, p=0.006).
About a quarter of patients admitted with HF or RD persist with severe dyspnoea at discharge. Opioids are probably underused. HF patients have less dyspnoea than patients with RD but present worse quality of life.
呼吸困难是心力衰竭(HF)和呼吸系统疾病(RD)患者入院时的一种致残症状。本研究的主要目的是评估入院时和出院时的呼吸困难强度及其与生活质量的关系。我们还描述了 HF 和 RD 中呼吸困难的管理、强度和演变。
在这项描述性、横断面研究中,我们前瞻性地纳入了 4 个月内因失代偿性 HF 和慢性阻塞性肺疾病(COPD)/肺纤维化而入院的所有患者。在出院时进行了量化呼吸困难(数字评分量表 1-10)和生活质量(EuroQoL 5d)的调查。
共纳入 258 例患者:190 例(73.6%)为 HF,68 例(26.4%)为 RD(62 例 COPD 和 6 例肺纤维化)。平均年龄为 74.0±1.2 岁,157 例(60.6%)为男性。入院前呼吸困难评分为 7.5±0.1。RD 患者入院时和出院时的呼吸困难均大于 HF 患者(分别为 8.1±0.2 与 7.3±0.2,p=0.01 和 3.2±0.3 与 2.0±0.2,p=0.0001)。RD 患者出院时呼吸困难严重程度(≥5)的发生率也更高(23[34.3%]与 36[19.1%],p=0.02)。41 例(15.9%)使用了阿片类药物,平均剂量为 8.7±0.8mg 吗啡当量日剂量。HF 患者的 EuroQoL 5d 评分比 RD 患者差,原因是活动能力问题(118[62.1%]与 28[41.8%],p=0.004)和视觉模拟评分较低(57.9±1.6 与 65.6±1.0,p=0.006)。
约四分之一因 HF 或 RD 入院的患者出院时仍存在严重呼吸困难。阿片类药物可能使用不足。HF 患者的呼吸困难程度低于 RD 患者,但生活质量更差。