Nuvoli Susanna, Spanu Angela, Piras Maria Rita, Nieddu Antonio, Mulas Aldo, Rocchitta Gaia, Galleri Grazia, Serra Pier Andrea, Madeddu Giuseppe
Nuclear Medicine Unit Neurology Unit, Department of Clinical and Experimental Medicine, University of Sassari, Sassari, Italy Geriatric Unit, Policlinico Sassarese Pharmacology Unit Internal Medicine Unit, Department of Clinical and Experimental Medicine, University of Sassari, Sassari, Italy.
Medicine (Baltimore). 2017 May;96(21):e6967. doi: 10.1097/MD.0000000000006967.
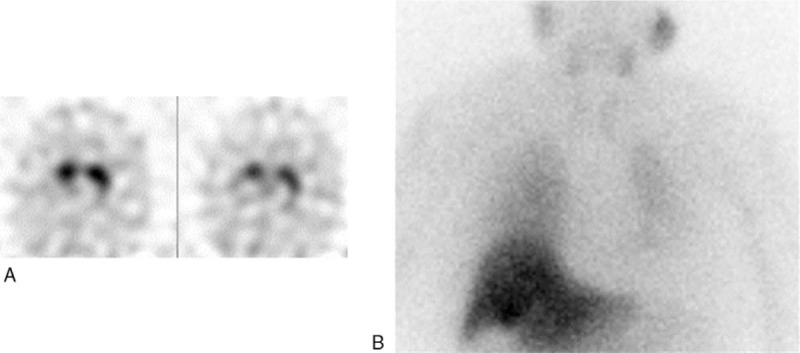
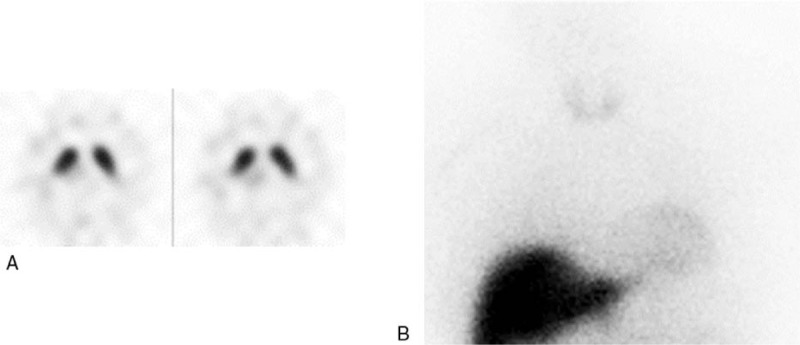
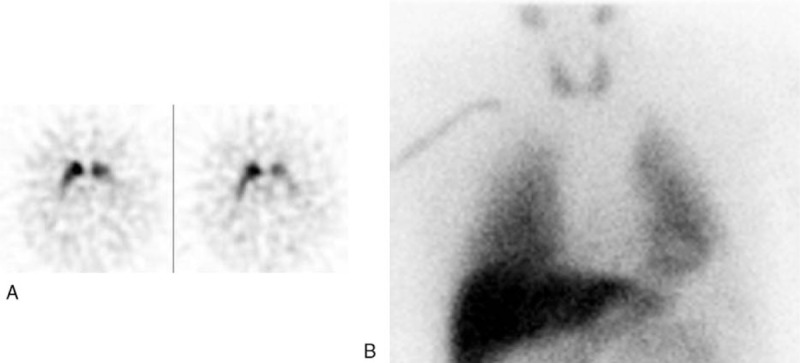
We evaluated the clinical usefulness of the combined use of I-ioflupane brain single photon emission computed tomography (SPECT) and I-metaiodobenzylguanidine (MIBG) cardiac scintigraphy in discriminating uncertain parkinsonism with vascular lesions in striatal nuclei at magnetic resonance imaging (MRI). Forty-three consecutive patients with uncertain parkinsonism and vascular lesions at MRI in striatal nuclei were retrospectively evaluated; the uncertain differential diagnosis was between Parkinson's disease and vascular parkinsonism (PD/VP) in 22 patients, between PD and other neurodegenerative parkinsonism (PD/PS) in 11 patients and between Lewy body dementia and Alzheimer disease (LBD/AD) in the remaining 10 cases. All patients underwent I-ioflupane SPECT with striatal dopaminergic activity determination as binding potentials (BP; cut-off: 3.3). I-MIBG cardiac planar scintigraphy was performed 2 weeks later, in early (15 minutes) and delayed (240 minutes) phases also calculating heart to mediastinum (H/M) ratio (cut-off: 1.56). I-Ioflupane uptake was normal in 9 patients with BP values >3.3, while it was reduced in 34/43 cases with BP values <3.3 at least in one of the striatal nuclei. I-MIBG uptake was normal in 21/43 patients (5 of whom with normal and 16 with I-ioflupane striatal defects) showing the H/M ratio >1.56 in all cases; the uptake was reduced in 22/43 cases, (4 of whom were normal and 18 were with I-ioflupane striatal defects) with the H/M ratio <1.56 in all cases. No statistical differences were found when early and delayed H/M ratios were mutually compared. Combining the 2 radioisotopic procedures, a more reliable diagnosis was achieved in 39/43 cases properly classifying 13 PD, 10 VP, 7 PS, 5 LBD, and 4 AD. However, the diagnosis remained uncertain in four patients with normal I-ioflupane and reduced I-MIBG uptake. The results of the present study confirmed that in uncertain parkinsonian syndromes associated with vascular lesions in striatal nuclei, brain I-ioflupane SPECT alone did not prove able to discriminate between the different forms of disease. Only the association with I-MIBG cardiac scintigraphy, also with the early acquisition alone, allowed the most appropriate diagnosis in 90.7% of our cases. However, patients with normal I-ioflupane and reduced I-I-MIBG uptakes need a close clinical and instrumental follow-up as sympathetic damage could precede striatal disorders in the early stage of PD and LBD.
我们评估了联合使用I-碘氟潘脑单光子发射计算机断层扫描(SPECT)和I-间碘苄胍(MIBG)心脏闪烁显像在鉴别磁共振成像(MRI)显示纹状体核有血管病变的不确定性帕金森综合征中的临床实用性。对43例连续的MRI显示纹状体核有血管病变的不确定性帕金森综合征患者进行了回顾性评估;22例患者的不确定性鉴别诊断为帕金森病和血管性帕金森综合征(PD/VP)之间,11例患者为帕金森病和其他神经退行性帕金森综合征(PD/PS)之间,其余10例为路易体痴呆和阿尔茨海默病(LBD/AD)之间。所有患者均接受I-碘氟潘SPECT检查,以纹状体多巴胺能活性测定作为结合电位(BP;临界值:3.3)。2周后进行I-MIBG心脏平面闪烁显像,在早期(15分钟)和延迟期(240分钟)也计算心脏与纵隔(H/M)比值(临界值:1.56)。9例BP值>3.3的患者I-碘氟潘摄取正常,但43例中有34例至少在一个纹状体核中BP值<3.3,其摄取减少。43例患者中有21例(其中5例I-碘氟潘摄取正常,16例有I-碘氟潘纹状体缺损)I-MIBG摄取正常,所有病例H/M比值>1.56;43例中有22例(其中4例正常,18例有I-碘氟潘纹状体缺损)摄取减少,所有病例H/M比值<1.56。早期和延迟H/M比值相互比较时未发现统计学差异。将这两种放射性同位素检查方法结合起来,43例中有39例获得了更可靠的诊断,正确分类为13例帕金森病、10例血管性帕金森综合征、7例其他神经退行性帕金森综合征、5例路易体痴呆和4例阿尔茨海默病。然而,4例I-碘氟潘摄取正常但I-MIBG摄取减少的患者诊断仍不确定。本研究结果证实,在与纹状体核血管病变相关的不确定性帕金森综合征中,单独的脑I-碘氟潘SPECT不能区分不同形式的疾病。只有与I-MIBG心脏闪烁显像联合使用,即使仅进行早期采集,也能在我们90.7%的病例中做出最合适的诊断。然而,I-碘氟潘摄取正常但I-MIBG摄取减少的患者需要密切的临床和仪器随访,因为在帕金森病和路易体痴呆的早期阶段,交感神经损伤可能先于纹状体疾病出现。