Wanja Elizabeth, Achilla Rachel, Obare Peter, Adeny Rose, Moseti Caroline, Otieno Victor, Morang'a Collins, Murigi Ephantus, Nyamuni John, Monthei Derek R, Ogutu Bernhards, Buff Ann M
Malaria Diagnostics Center, U.S. Army Medical Research Directorate-Kenya, Box 54, Kisumu, 40100, Kenya.
Malaria Diagnostics Center, Kenya Medical Research Institute, Box 54, Kisumu, 40100, Kenya.
Malar J. 2017 May 25;16(1):221. doi: 10.1186/s12936-017-1856-2.
One objective of the Kenya National Malaria Strategy 2009-2017 is scaling access to prompt diagnosis and effective treatment. In 2013, a quality assurance (QA) pilot was implemented to improve accuracy of malaria diagnostics at selected health facilities in low-transmission counties of Kenya. Trends in malaria diagnostic and QA indicator performance during the pilot are described.
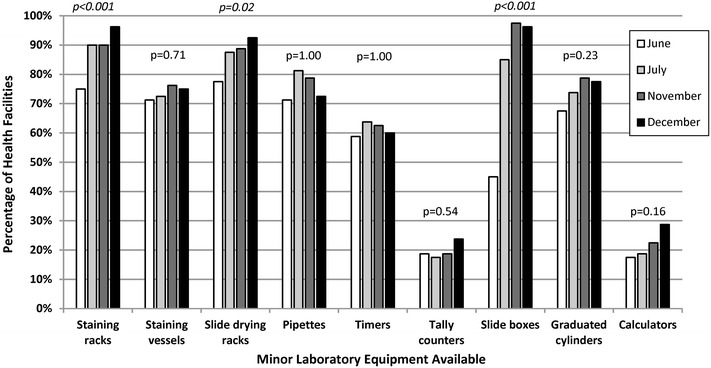
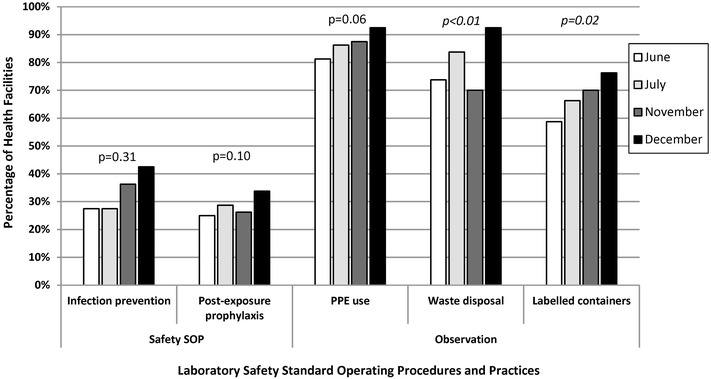
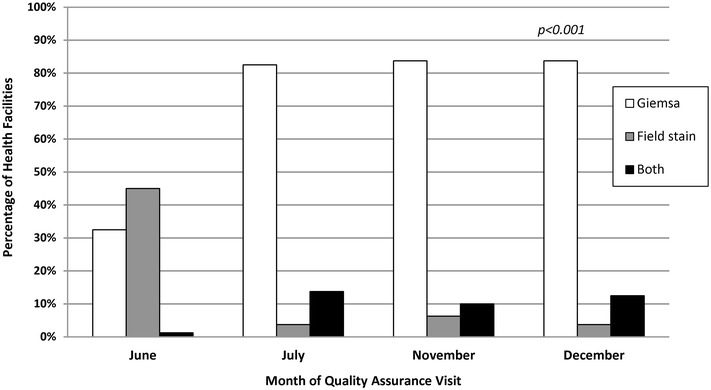
From June to December 2013, 28 QA officers provided on-the-job training and mentoring for malaria microscopy, malaria rapid diagnostic tests and laboratory QA/quality control (QC) practices over four 1-day visits at 83 health facilities. QA officers observed and recorded laboratory conditions and practices and cross-checked blood slides for malaria parasite presence, and a portion of cross-checked slides were confirmed by reference laboratories.
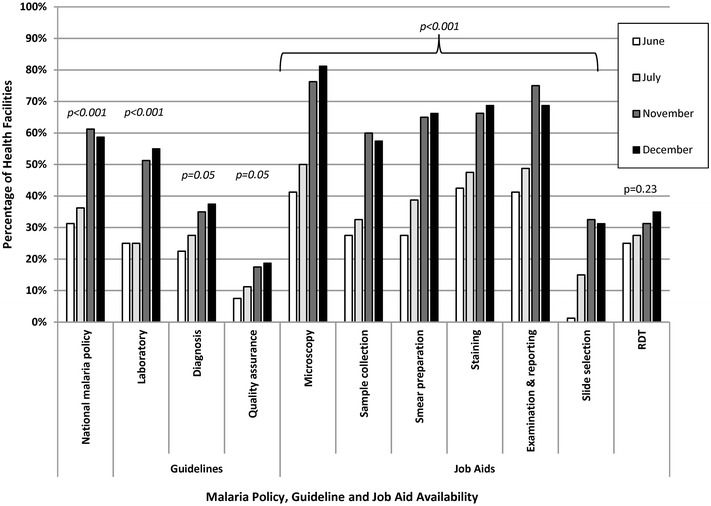
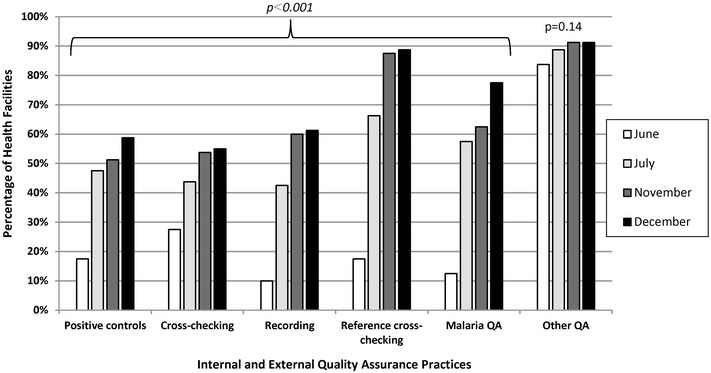
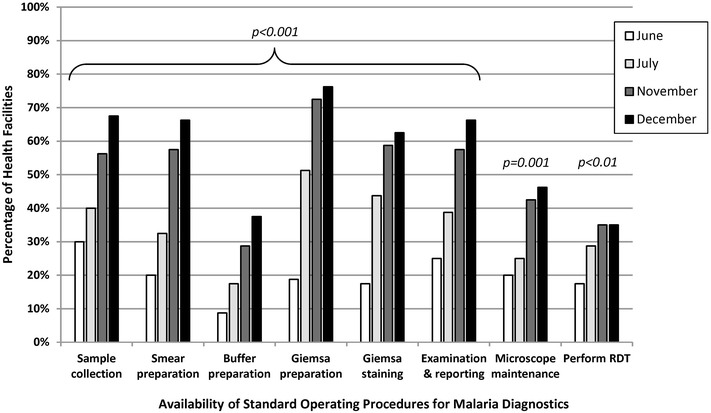
Eighty (96%) facilities completed the pilot. Among 315 personnel at pilot initiation, 13% (n = 40) reported malaria diagnostics training within the previous 12 months. Slide positivity ranged from 3 to 7%. Compared to the reference laboratory, microscopy sensitivity ranged from 53 to 96% and positive predictive value from 39 to 53% for facility staff and from 60 to 96% and 52 to 80%, respectively, for QA officers. Compared to reference, specificity ranged from 88 to 98% and negative predictive value from 98 to 99% for health-facility personnel and from 93 to 99% and 99%, respectively, for QA officers. The kappa value ranged from 0.48-0.66 for facility staff and 0.57-0.84 for QA officers compared to reference. The only significant test performance improvement observed for facility staff was for specificity from 88% (95% CI 85-90%) to 98% (95% CI 97-99%). QA/QC practices, including use of positive-control slides, internal and external slide cross-checking and recording of QA/QC activities, all increased significantly across the pilot (p < 0.001). Reference material availability also increased significantly; availability of six microscopy job aids and seven microscopy standard operating procedures increased by a mean of 32 percentage points (p < 0.001) and 38 percentage points (p < 0.001), respectively.
Significant gains were observed in malaria QA/QC practices over the pilot. However, these advances did not translate into improved accuracy of malaria diagnostic performance perhaps because of the limited duration of the QA pilot implementation.
《2009 - 2017年肯尼亚国家疟疾战略》的目标之一是扩大及时诊断和有效治疗的可及性。2013年,实施了一项质量保证(QA)试点,以提高肯尼亚低传播县选定卫生设施的疟疾诊断准确性。描述了试点期间疟疾诊断和质量保证指标的表现趋势。
2013年6月至12月,28名质量保证官员在83个卫生设施进行了4次为期1天的访问,就疟疾显微镜检查、疟疾快速诊断检测和实验室质量保证/质量控制(QC)实践提供在职培训和指导。质量保证官员观察并记录实验室条件和操作,交叉检查血涂片以确定是否存在疟原虫,一部分交叉检查的涂片由参考实验室进行确认。
80个(96%)设施完成了试点。在试点开始时的315名人员中,13%(n = 40)报告在过去12个月内接受过疟疾诊断培训。血涂片阳性率在3%至7%之间。与参考实验室相比,设施工作人员显微镜检查的敏感性在53%至96%之间,阳性预测值在39%至53%之间;质量保证官员的敏感性在60%至96%之间,阳性预测值在52%至80%之间。与参考相比,卫生设施人员的特异性在88%至98%之间,阴性预测值在98%至99%之间;质量保证官员的特异性在93%至99%之间,阴性预测值为99%。与参考相比,设施工作人员的kappa值在0.48 - 0.66之间,质量保证官员的kappa值在0.57 - 0.84之间。观察到设施工作人员唯一显著的检测性能改善是特异性从88%(95%可信区间85 - 90%)提高到98%(95%可信区间97 - 99%)。质量保证/质量控制实践,包括使用阳性对照涂片、内部和外部血涂片交叉检查以及质量保证/质量控制活动的记录,在整个试点期间均显著增加(p < 0.001)。参考材料的可用性也显著增加;六种显微镜操作辅助工具和七种显微镜标准操作规程的可用性平均分别增加了32个百分点(p < 0.001)和38个百分点(p < 0.001)。
在试点期间,疟疾质量保证/质量控制实践取得了显著进展。然而,这些进展并未转化为疟疾诊断性能准确性的提高,可能是因为质量保证试点实施的时间有限。