Cuttica Michael J, Bhatt Surya P, Rosenberg Sharon R, Beussink Lauren, Shah Sanjiv J, Smith Lewis J, Dransfield Mark T, Kalhan Ravi
Division of Pulmonary and Critical Care Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL.
Division of Pulmonary, Allergy & Critical Care Medicine, University of Alabama-Birmingham, Birmingham, AL.
Int J Chron Obstruct Pulmon Dis. 2017 May 12;12:1439-1446. doi: 10.2147/COPD.S131413. eCollection 2017.
The ratio of the diameter of the pulmonary artery (PA) to the diameter of the aorta (PA:A) on computed tomography (CT) imaging is associated with both COPD exacerbation and pulmonary hypertension. The mechanisms of PA enlargement in COPD are poorly understood.
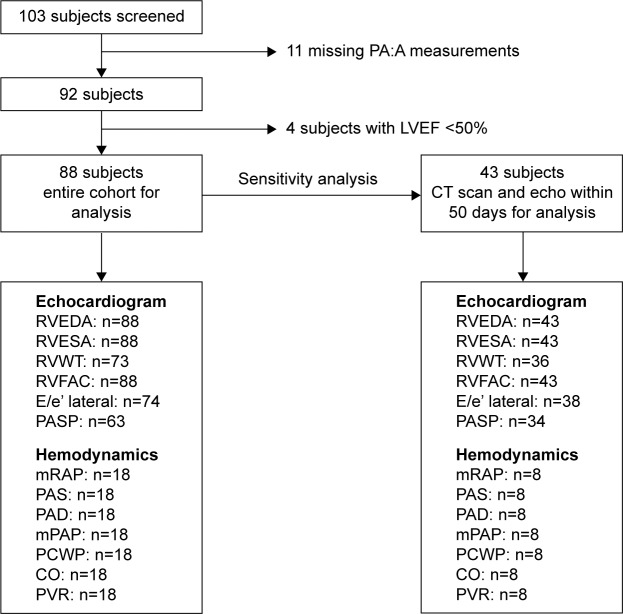
In this retrospective, single center study we evaluated pulmonary function, CT scans, right heart catheterizations, and echocardiography in 88 subjects with mild-to-moderately severe COPD. A sensitivity analysis was performed in 43 subjects in whom CT scan and echocardiogram were performed within 50 days of each other. To evaluate the association between PA:A ratio and echocardiographic parameters and hemodynamics, we performed simple correlations and multivariable linear regression analysis adjusting for lung function, age, sex, race, and diastolic function.
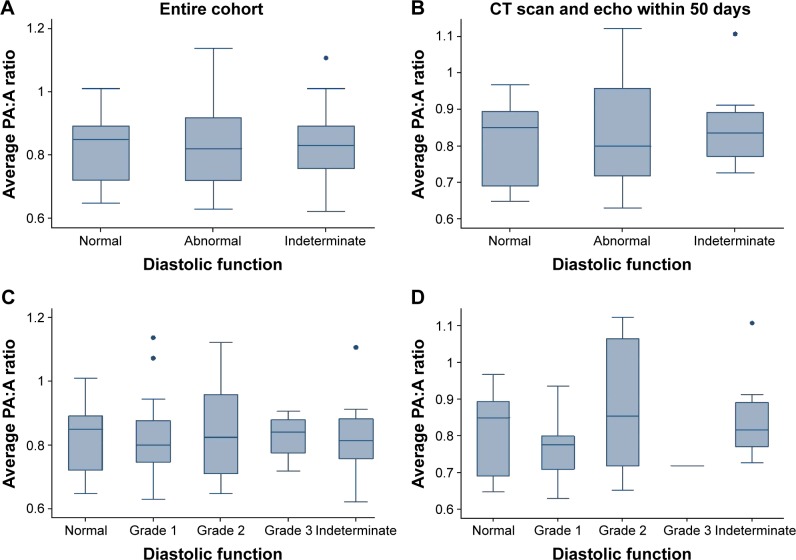
All subjects had preserved left ventricular (LV) systolic function (LV ejection fraction 62.7%±5.5%). Among them, 56.8% had evidence of diastolic dysfunction. There was no association between PA:A ratio and the presence of diastolic dysfunction. In a multivariable model, PA:A ratio was associated with right ventricular (RV) chamber size (β=0.015; <0.003), RV wall thickness (β=0.56; <0.002), and RV function (-0.49; =0.05). In the subgroup of subjects with testing within 50 days, the association with RV chamber size persisted (β=0.017; =0.04), as did the lack of association with diastolic function. PA:A ratio was also associated with elevated PA systolic pressures (=0.62; =0.006) and pulmonary vascular resistance (=0.46; =0.05), but not pulmonary arterial wedge pressure (=0.17; =0.5) in a subset of patients undergoing right heart catheterization.
In patients with mild-to-moderately severe COPD and preserved LV function, increased PA:A ratio occurs independent of LV diastolic dysfunction. Furthermore, the PA:A ratio is associated with right heart structure and function changes, as well as pulmonary hemodynamics. These findings indicate that PA:A ratio is a marker of intrinsic pulmonary vascular changes rather than impaired LV filling.
计算机断层扫描(CT)成像中肺动脉(PA)直径与主动脉直径之比(PA:A)与慢性阻塞性肺疾病(COPD)急性加重和肺动脉高压均相关。COPD中PA增大的机制尚不清楚。
在这项回顾性单中心研究中,我们评估了88例轻至中度严重COPD患者的肺功能、CT扫描、右心导管检查和超声心动图。对43例在50天内先后进行CT扫描和超声心动图检查的患者进行了敏感性分析。为了评估PA:A比值与超声心动图参数及血流动力学之间的关联,我们进行了简单相关性分析和多变量线性回归分析,并对肺功能、年龄、性别、种族和舒张功能进行了校正。
所有患者左心室(LV)收缩功能均正常(LV射血分数62.7%±5.5%)。其中,56.8%有舒张功能障碍的证据。PA:A比值与舒张功能障碍的存在无关。在多变量模型中,PA:A比值与右心室(RV)腔大小(β=0.015;P<0.003)、RV壁厚度(β=0.56;P<0.002)和RV功能(β=-0.49;P=0.05)相关。在50天内进行检查的患者亚组中,与RV腔大小的关联仍然存在(β=0.017;P=0.04),与舒张功能的无关联也依然存在。在接受右心导管检查的一部分患者中,PA:A比值还与PA收缩压升高(β=0.62;P=0.006)和肺血管阻力升高(β=0.46;P=0.05)相关,但与肺动脉楔压无关(β=0.17;P=0.5)。
在轻至中度严重COPD且LV功能正常的患者中,PA:A比值升高独立于LV舒张功能障碍而发生。此外,PA:A比值与右心结构和功能变化以及肺血流动力学相关。这些发现表明,PA:A比值是肺血管内在变化的标志物,而非LV充盈受损的标志物。