Lisonkova Sarka, Potts Jayson, Muraca Giulia M, Razaz Neda, Sabr Yasser, Chan Wee-Shian, Kramer Michael S
Department of Obstetrics and Gynaecology, University of British Columbia and Children's and Women's Health Centre of British Columbia, Vancouver, British Columbia, Canada.
School of Population and Public Health, University of British Columbia, Vancouver, British Columbia, Canada.
PLoS Med. 2017 May 30;14(5):e1002307. doi: 10.1371/journal.pmed.1002307. eCollection 2017 May.
One of the United Nations' Millennium Development Goals of 2000 was to reduce maternal mortality by 75% in 15 y; however, this challenge was not met by many industrialized countries. As average maternal age continues to rise in these countries, associated potentially life-threatening severe maternal morbidity has been understudied. Our primary objective was to examine the associations between maternal age and severe maternal morbidities. The secondary objective was to compare these associations with those for adverse fetal/infant outcomes.
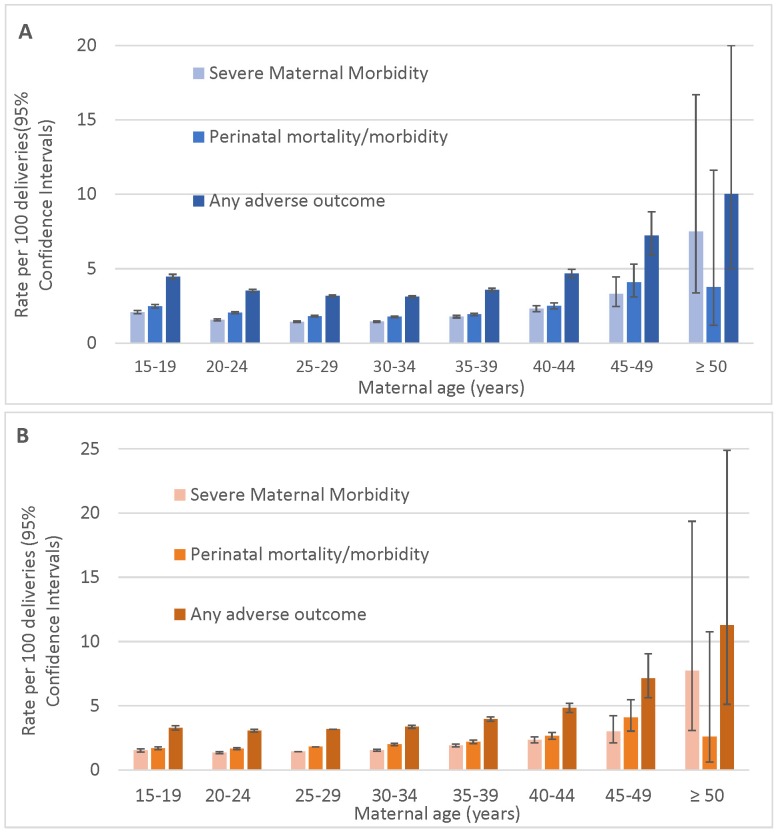
This was a population-based retrospective cohort study, including all singleton births to women residing in Washington State, US, 1 January 2003-31 December 2013 (n = 828,269). We compared age-specific rates of maternal mortality/severe morbidity (e.g., obstetric shock) and adverse fetal/infant outcomes (e.g., perinatal death). Logistic regression was used to adjust for parity, body mass index, assisted conception, and other potential confounders. We compared crude odds ratios (ORs) and adjusted ORs (AORs) and risk differences and their 95% CIs. Severe maternal morbidity was significantly higher among teenage mothers than among those 25-29 y (crude OR = 1.5, 95% CI 1.5-1.6) and increased exponentially with maternal age over 39 y, from OR = 1.2 (95% CI 1.2-1.3) among women aged 35-39 y to OR = 5.4 (95% CI 2.4-12.5) among women aged ≥50 y. The elevated risk of severe morbidity among teen mothers disappeared after adjustment for confounders, except for maternal sepsis (AOR = 1.2, 95% CI 1.1-1.4). Adjusted rates of severe morbidity remained increased among mothers ≥35 y, namely, the rates of amniotic fluid embolism (AOR = 8.0, 95% CI 2.7-23.7) and obstetric shock (AOR = 2.9, 95% CI 1.3-6.6) among mothers ≥40 y, and renal failure (AOR = 15.9, 95% CI 4.8-52.0), complications of obstetric interventions (AOR = 4.7, 95% CI 2.3-9.5), and intensive care unit (ICU) admission (AOR = 4.8, 95% CI 2.0-11.9) among those 45-49 y. The adjusted risk difference in severe maternal morbidity compared to mothers 25-29 y was 0.9% (95% CI 0.7%-1.2%) for mothers 40-44 y, 1.6% (95% CI 0.7%-2.8%) for mothers 45-49 y, and 6.4% for mothers ≥50 y (95% CI 1.7%-18.2%). Similar associations were observed for fetal and infant outcomes; neonatal mortality was elevated in teen mothers (AOR = 1.5, 95% CI 1.2-1.7), while mothers over 29 y had higher risk of stillbirth. The rate of severe maternal morbidity among women over 49 y was higher than the rate of mortality/serious morbidity of their offspring. Despite the large sample size, statistical power was insufficient to examine the association between maternal age and maternal death or very rare severe morbidities.
Maternal age-specific incidence of severe morbidity varied by outcome. Older women (≥40 y) had significantly elevated rates of some of the most severe, potentially life-threatening morbidities, including renal failure, shock, acute cardiac morbidity, serious complications of obstetric interventions, and ICU admission. These results should improve counselling to women who contemplate delaying childbirth until their forties and provide useful information to their health care providers. This information is also useful for preventive strategies to lower maternal mortality and severe maternal morbidity in developed countries.
2000年联合国千年发展目标之一是在15年内将孕产妇死亡率降低75%;然而,许多工业化国家并未实现这一目标。随着这些国家孕产妇平均年龄持续上升,与之相关的潜在危及生命的严重孕产妇发病率一直未得到充分研究。我们的主要目标是研究孕产妇年龄与严重孕产妇疾病之间的关联。次要目标是将这些关联与不良胎儿/婴儿结局的关联进行比较。
这是一项基于人群的回顾性队列研究,纳入了2003年1月1日至2013年12月31日居住在美国华盛顿州的所有单胎分娩妇女(n = 828,269)。我们比较了特定年龄组的孕产妇死亡率/严重发病率(如产科休克)和不良胎儿/婴儿结局(如围产期死亡)。采用逻辑回归调整胎次、体重指数、辅助受孕及其他潜在混杂因素。我们比较了粗比值比(OR)和调整后的比值比(AOR)以及风险差异及其95%置信区间。青少年母亲的严重孕产妇发病率显著高于25 - 29岁的母亲(粗OR = 1.5,95% CI 1.5 - 1.6),且随着孕产妇年龄超过39岁呈指数上升,从35 - 39岁妇女的OR = 1.2(95% CI 1.2 - 1.3)增至≥50岁妇女的OR = 5.4(95% CI 2.4 - 12.5)。除孕产妇败血症外(AOR = 1.2,95% CI 1.1 - 1.4),调整混杂因素后青少年母亲严重发病率升高的风险消失。≥35岁母亲的严重发病率调整率仍升高,即≥40岁母亲的羊水栓塞率(AOR = 8.0,95% CI 2.7 - 23.7)和产科休克率(AOR = 2.9,95% CI 1.3 - 6.6),以及45 - 49岁母亲的肾衰竭率(AOR = 15.9,95% CI 4.8 - 52.0)、产科干预并发症率(AOR = 4.7,95% CI 2.3 - 9.5)和重症监护病房(ICU)入住率(AOR = 4.8,95% CI 2.0 - 11.9)。与25 - 29岁母亲相比,40 - 44岁母亲严重孕产妇发病率的调整风险差异为0.9%(95% CI 0.7% - 1.2%),45 - 49岁母亲为1.6%(95% CI 0.7% - 2.8%),≥50岁母亲为6.4%(95% CI 1.7% - 18.2%)。胎儿和婴儿结局也观察到类似关联;青少年母亲的新生儿死亡率升高(AOR = 1.5,95% CI 1.2 - 1.7),而29岁以上母亲的死产风险更高。49岁以上妇女的严重孕产妇发病率高于其后代的死亡率/严重发病率。尽管样本量很大,但统计效能不足以检验孕产妇年龄与孕产妇死亡或非常罕见的严重疾病之间的关联。
严重发病率的孕产妇年龄特异性发病率因结局而异。年龄较大的妇女(≥40岁)某些最严重的、潜在危及生命的疾病发病率显著升高,包括肾衰竭、休克、急性心脏疾病、产科干预的严重并发症和ICU入住。这些结果应改善对考虑推迟生育至四十多岁的妇女的咨询,并为其医疗保健提供者提供有用信息。这些信息对于发达国家降低孕产妇死亡率和严重孕产妇发病率的预防策略也很有用。