Vieira Matias C, McCowan Lesley M E, Gillett Alexandra, Poston Lucilla, Fyfe Elaine, Dekker Gustaaf A, Baker Philip N, Walker James J, Kenny Louise C, Pasupathy Dharmintra
Division of Women's Health, Women's Health Academic Centre, King's College London and King's Health Partners, London, United Kingdom.
Núcleo de Formação Específica em Ginecologia e Obstetrícia, Escola de Medicina, Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, Brazil.
PLoS One. 2017 Jun 1;12(6):e0178484. doi: 10.1371/journal.pone.0178484. eCollection 2017.
To develop a prediction model for term infants born large for gestational age (LGA) by customised birthweight centiles.
International prospective cohort of nulliparous women with singleton pregnancy recruited to the Screening for Pregnancy Endpoints (SCOPE) study. LGA was defined as birthweight above the 90th customised centile, including adjustment for parity, ethnicity, maternal height and weight, fetal gender and gestational age. Clinical risk factors, ultrasound parameters and biomarkers at 14-16 or 19-21 weeks were combined into a prediction model for LGA infants at term using stepwise logistic regression in a training dataset. Prediction performance was assessed in a validation dataset using area under the Receiver Operating Characteristics curve (AUC) and detection rate at fixed false positive rates.
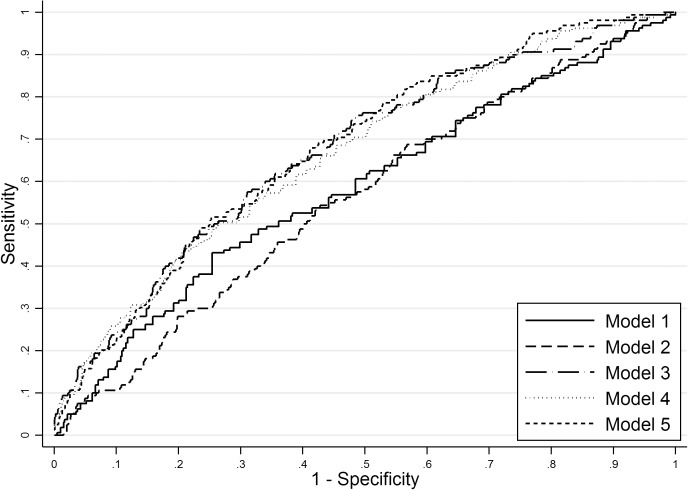
The prevalence of LGA at term was 8.8% (n = 491/5628). Clinical and ultrasound factors selected in the prediction model for LGA infants were maternal birthweight, gestational weight gain between 14-16 and 19-21 weeks, and fetal abdominal circumference, head circumference and uterine artery Doppler resistance index at 19-21 weeks (AUC 0.67; 95%CI 0.63-0.71). Sensitivity of this model was 24% and 49% for a fixed false positive rate of 10% and 25%, respectively. The addition of biomarkers resulted in selection of random glucose, LDL-cholesterol, vascular endothelial growth factor receptor-1 (VEGFR1) and neutrophil gelatinase-associated lipocalin (NGAL), but with minimal improvement in model performance (AUC 0.69; 95%CI 0.65-0.73). Sensitivity of the full model was 26% and 50% for a fixed false positive rate of 10% and 25%, respectively.
Prediction of LGA infants at term has limited diagnostic performance before 22 weeks but may have a role in contingency screening in later pregnancy.
通过定制出生体重百分位数来建立足月儿大于胎龄儿(LGA)的预测模型。
纳入国际前瞻性队列研究“妊娠结局筛查(SCOPE)研究”中的初产妇单胎妊娠妇女。LGA定义为出生体重高于第90定制百分位数,包括对产次、种族、母亲身高和体重、胎儿性别及孕周进行校正。将孕14 - 16周或19 - 21周时的临床危险因素、超声参数和生物标志物,在一个训练数据集中使用逐步逻辑回归法整合为足月儿LGA的预测模型。在一个验证数据集中,使用受试者操作特征曲线下面积(AUC)和固定假阳性率下的检测率评估预测性能。
足月儿LGA的患病率为8.8%(n = 491/5628)。LGA婴儿预测模型中选择的临床和超声因素为母亲出生体重、孕14 - 16周和19 - 21周之间的孕期体重增加,以及孕19 - 21周时的胎儿腹围、头围和子宫动脉多普勒阻力指数(AUC 0.67;95%CI 0.63 - 0.71)。对于固定假阳性率为10%和25%,该模型的敏感性分别为24%和49%。添加生物标志物后,随机血糖、低密度脂蛋白胆固醇、血管内皮生长因子受体 - 1(VEGFR1)和中性粒细胞明胶酶相关脂质运载蛋白(NGAL)被选中,但模型性能改善极小(AUC 0.69;95%CI 0.65 - 0.73)。对于固定假阳性率为10%和25%,完整模型的敏感性分别为26%和50%。
在孕22周前预测足月儿LGA的诊断性能有限,但可能在妊娠后期的应急筛查中发挥作用。