The Generation R Study Group, Erasmus MC, University Medical Center, PO Box 2040, 3000, CA, Rotterdam, The Netherlands.
Department of Pediatrics, Sophia's Children's Hospital, Erasmus MC, University Medical Center, Rotterdam, the Netherlands.
BMC Pregnancy Childbirth. 2022 Feb 28;22(1):165. doi: 10.1186/s12884-022-04497-2.
Suboptimal maternal health already from preconception onwards is strongly linked to an increased risk of birth complications. To enable identification of women at risk of birth complications, we aimed to develop a prediction model for birth complications using maternal preconception socio-demographic, lifestyle, medical history and early-pregnancy clinical characteristics in a general population.
In a population-based prospective cohort study among 8340 women, we obtained information on 33 maternal characteristics at study enrolment in early-pregnancy. These characteristics covered the preconception period and first half of pregnancy (< 21 weeks gestation). Preterm birth was < 37 weeks gestation. Small-for-gestational-age (SGA) and large-for-gestational-age (LGA) at birth were gestational-age-adjusted birthweight in the lowest or highest decile, respectively. Because of their co-occurrence, preterm birth and SGA were combined into a composite outcome.
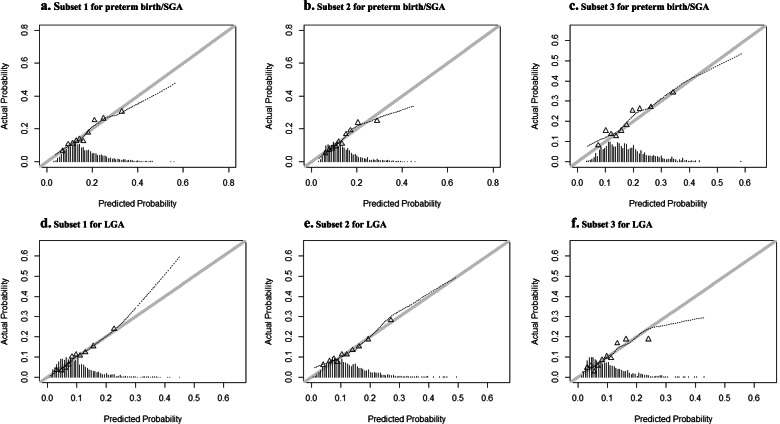
The basic preconception model included easy obtainable maternal characteristics in the preconception period including age, ethnicity, parity, body mass index and smoking. This basic preconception model had an area under the receiver operating characteristics curve (AUC) of 0.63 (95% confidence interval (CI) 0.61 to 0.65) and 0.64 (95% CI 0.62 to 0.66) for preterm birth/SGA and LGA, respectively. Further extension to more complex models by adding maternal socio-demographic, lifestyle, medical history and early-pregnancy clinical characteristics led to small, statistically significant improved models. The full model for prediction of preterm birth/SGA had an AUC 0.66 (95% CI 0.64 to 0.67) with a sensitivity of 22% at a 90% specificity. The full model for prediction of LGA had an AUC of 0.67 (95% CI 0.65 to 0.69) with sensitivity of 28% at a 90% specificity. The developed models had a reasonable level of calibration within highly different socio-economic subsets of our population and predictive performance for various secondary maternal, delivery and neonatal complications was better than for primary outcomes.
Prediction of birth complications is limited when using maternal preconception and early-pregnancy characteristics, which can easily be obtained in clinical practice. Further improvement of the developed models and subsequent external validation is needed.
从受孕前开始,孕产妇健康状况欠佳与分娩并发症风险增加密切相关。为了识别分娩并发症风险较高的女性,我们旨在使用一般人群中孕产妇受孕前的社会人口统计学、生活方式、病史和孕早期临床特征来建立分娩并发症预测模型。
在一项基于人群的前瞻性队列研究中,我们对 8340 名女性在孕早期的 33 项孕产妇特征进行了研究。这些特征涵盖了受孕前阶段和妊娠前半段(<21 周妊娠)。早产是指妊娠 37 周前分娩。出生时小于胎龄儿(SGA)和大于胎龄儿(LGA)是指按胎龄调整的出生体重处于最低或最高十分位数。由于它们的同时发生,早产和 SGA 被合并为一个复合结局。
基本的受孕前模型包括受孕前阶段易于获得的孕产妇特征,包括年龄、种族、产次、体重指数和吸烟。该基本受孕前模型对早产/SGA 和 LGA 的受试者工作特征曲线下面积(AUC)分别为 0.63(95%置信区间(CI)0.61 至 0.65)和 0.64(95%CI 0.62 至 0.66)。通过添加孕产妇社会人口统计学、生活方式、病史和孕早期临床特征,进一步扩展到更复杂的模型,导致模型略有改善,但具有统计学意义。用于预测早产/SGA 的完整模型 AUC 为 0.66(95%CI 0.64 至 0.67),特异性为 90%时的灵敏度为 22%。用于预测 LGA 的完整模型 AUC 为 0.67(95%CI 0.65 至 0.69),特异性为 90%时的灵敏度为 28%。在我们人群中高度不同的社会经济亚组中,所开发的模型具有合理的校准水平,并且对各种次要的孕产妇、分娩和新生儿并发症的预测性能优于主要结局。
使用在临床实践中易于获得的孕产妇受孕前和孕早期特征来预测分娩并发症的效果有限。需要进一步改进和外部验证所开发的模型。