Division of Infectious Diseases and International Health, University of Virginia, Charlottesville.
Haydom Global Health Research Centre, Haydom Lutheran Hospital, and.
Clin Infect Dis. 2017 Oct 1;65(7):1144-1151. doi: 10.1093/cid/cix494.
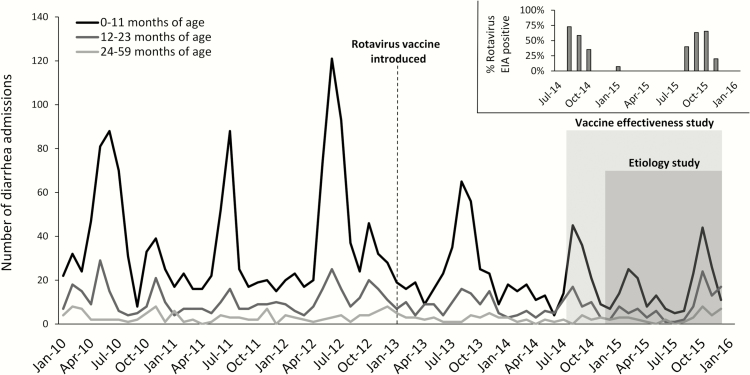
No data are available on the etiology of diarrhea requiring hospitalization after rotavirus vaccine introduction in Africa. The monovalent rotavirus vaccine was introduced in Tanzania on 1 January 2013. We performed a vaccine impact and effectiveness study as well as a quantitative polymerase chain reaction (qPCR)-based etiology study at a rural Tanzanian hospital.
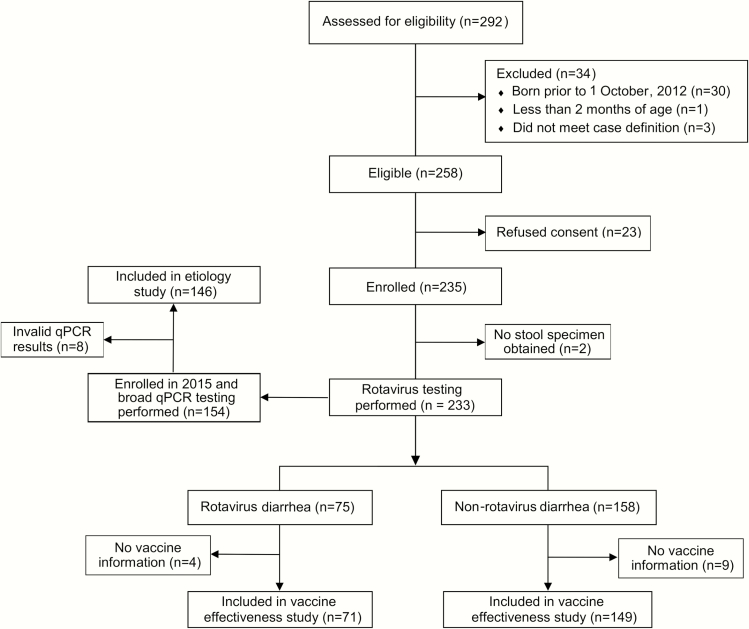
We obtained data on admissions among children <5 years to Haydom Lutheran Hospital between 1 January 2010 and 31 December 2015 and estimated the impact of vaccine introduction on all-cause diarrhea admissions. We then performed a vaccine effectiveness study using the test-negative design. Finally, we tested diarrheal specimens during 2015 by qPCR for a broad range of enteropathogens and calculated pathogen-specific attributable fractions (AFs).
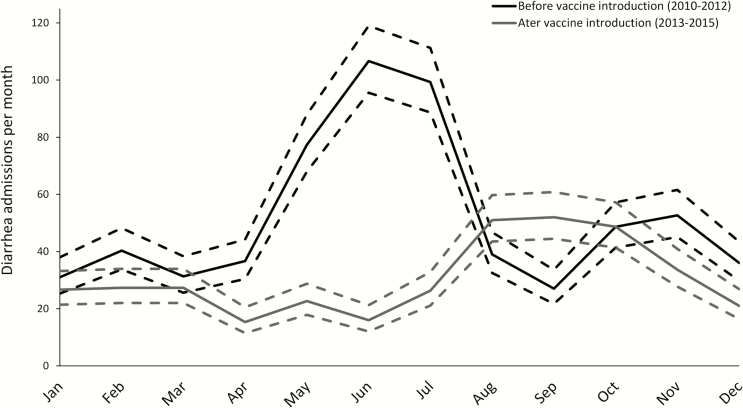
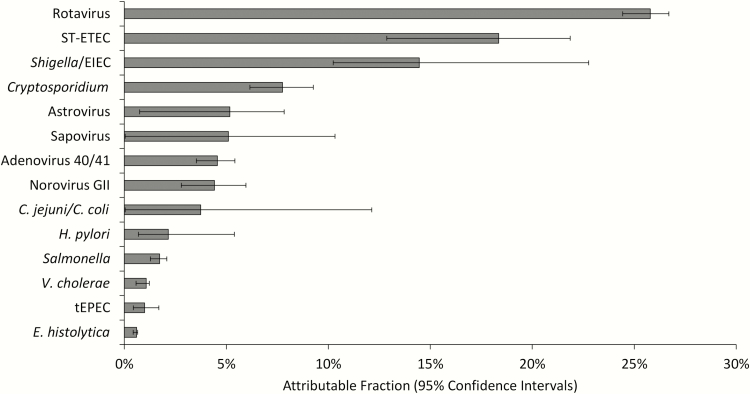
Vaccine introduction was associated with a 44.9% (95% confidence interval [CI], 17.6%-97.4%) reduction in diarrhea admissions in 2015, as well as delay of the rotavirus season. The effectiveness of 2 doses of vaccine was 74.8% (95% CI, -8.2% to 94.1%) using an enzyme immunoassay-based case definition and 85.1% (95% CI, 26.5%-97.0%) using a qPCR-based case definition. Among 146 children enrolled in 2015, rotavirus remained the leading etiology of diarrhea requiring hospitalization (AF, 25.8% [95% CI, 24.4%-26.7%]), followed by heat-stable enterotoxin-producing Escherichia coli (AF, 18.4% [95% CI, 12.9%-21.9%]), Shigella/enteroinvasive E. coli (AF, 14.5% [95% CI, 10.2%-22.8%]), and Cryptosporidium (AF, 7.9% [95% CI, 6.2%-9.3%]).
Despite the clear impact of vaccine introduction in this setting, rotavirus remained the leading etiology of diarrhea requiring hospitalization. Further efforts to maximize vaccine coverage and improve vaccine performance in these settings are warranted.
在引入轮状病毒疫苗后,非洲有关腹泻住院病因的数据尚不清楚。单价轮状病毒疫苗于 2013 年 1 月 1 日在坦桑尼亚引入。我们在坦桑尼亚的一家农村医院进行了疫苗效果和基于定量聚合酶链反应(qPCR)的病因学研究。
我们获得了 2010 年 1 月 1 日至 2015 年 12 月 31 日期间,Haydom Lutheran 医院 5 岁以下儿童住院数据,并估计了疫苗引入对所有病因腹泻住院的影响。然后,我们使用测试阴性设计进行了疫苗有效性研究。最后,我们在 2015 年使用 qPCR 对腹泻标本进行了广泛的肠道病原体检测,并计算了病原体特异性归因分数(AFs)。
2015 年,疫苗引入与腹泻住院减少 44.9%(95%置信区间 [CI],17.6%-97.4%)相关,并使轮状病毒流行季节延迟。使用酶免疫测定为基础的病例定义,两剂疫苗的有效性为 74.8%(95%CI,-8.2%至 94.1%),使用 qPCR 为基础的病例定义为 85.1%(95%CI,26.5%-97.0%)。在 2015 年纳入的 146 名儿童中,轮状病毒仍然是导致腹泻住院的主要病因(AF,25.8%[95%CI,24.4%-26.7%]),其次是耐热肠毒素产生大肠杆菌(AF,18.4%[95%CI,12.9%-21.9%]),志贺菌/肠侵袭性大肠杆菌(AF,14.5%[95%CI,10.2%-22.8%])和隐孢子虫(AF,7.9%[95%CI,6.2%-9.3%])。
尽管该环境中疫苗引入的效果明显,但轮状病毒仍然是导致腹泻住院的主要病因。需要进一步努力提高疫苗覆盖率并改善这些环境中的疫苗效果。