Hawkins Robert B, Mehaffey J Hunter, Narahari Adishesh K, Jain Amit, Ghanta Ravi K, Kron Irving L, Kern John A, Upchurch Gilbert R
Division of Thoracic and Cardiovascular Surgery, Department of Surgery, University of Virginia, Charlottesville, Va.
Division of Vascular Surgery, Department of Surgery, University of Cincinnati, Cincinnati, Ohio.
J Vasc Surg. 2017 Nov;66(5):1357-1363. doi: 10.1016/j.jvs.2017.03.420. Epub 2017 May 31.
Complex Crawford extent II thoracoabdominal aortic aneurysms (TAAAs) can be treated in a hybrid manner with proximal thoracic endovascular aneurysm repair, followed by staged distal open thoracoabdominal repair. This study evaluated the outcomes and health care-associated value of this new method compared with traditional open repair over 10 years.
A prospectively collected database was used to identify all patients with an extent II TAAA undergoing repair at a single institution between 2005 and 2015. Patient characteristics, postoperative outcomes, and incidence of major adverse events (MAEs; renal failure, spinal cord ischemia, death) were compared. After adjusting for time since surgery, value was analyzed looking at quality (1/MAE) divided by cost (total health system cost). This was multiplied by a constant to set the value of open TAAA repair to 100.
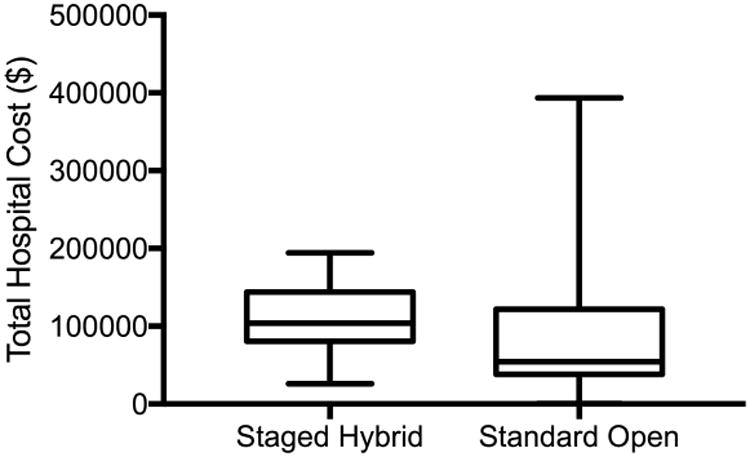
A total of 113 consecutive patients underwent extent II TAAA repairs, of whom 25 (22.1%) had a staged hybrid approach with a median of 129 days between procedures. No baseline differences in demographic or comorbidity variables existed between groups (P > .05). The hybrid group had shorter operative time (255 vs 306 minutes; P = .01), shorter postoperative length of stay (10.1 vs 13.3 days; P = .02), and reduced blood loss (1300 vs 2600 mL; P = .01) at the time of open operation. Despite higher rates of acute kidney injury in the hybrid group (76.0% vs 51.1%; P = .03), there was no difference in renal failure (8.0% vs 4.5%; P = .84). The incidence of MAEs was lower in the staged hybrid group (20.0% vs 48.9%; P = .01), without a difference in hospital mortality (4.0% vs 3.4%; P = .89). Median total cost was higher in the hybrid group ($112,920 vs $72,037; P = .003). Value was improved in the hybrid group by 56% using mean cost and 178% by median cost.
The 20% MAE rate associated with staged hybrid repair of extent II TAAA was significantly decreased compared with open repair, with a relative reduction of >50%. Despite higher total hospital costs, staged hybrid repair had 56% to 178% higher health care-related value compared with standard open repair. In an era of increasing focus on costs and quality, staged hybrid repair of extensive TAAAs is associated with fewer complications than open TAAA repair, resulting in a good value investment from a resource utilization perspective.
复杂的克劳福德II型胸腹主动脉瘤(TAAA)可以采用杂交方式治疗,即先进行近端胸段血管腔内动脉瘤修复术,随后分期进行远端开放性胸腹修复术。本研究评估了这种新方法与传统开放性修复术相比在10年期间的疗效及医疗保健相关价值。
使用前瞻性收集的数据库,确定2005年至2015年间在单一机构接受II型TAAA修复术的所有患者。比较患者特征、术后结果及主要不良事件(MAE;肾衰竭、脊髓缺血、死亡)的发生率。在调整术后时间后,分析价值,即质量(1/MAE)除以成本(医疗系统总成本)。将其乘以一个常数,以使开放性TAAA修复术的价值设定为100。
共有113例连续患者接受了II型TAAA修复术,其中25例(22.1%)采用分期杂交方法,两次手术之间的中位间隔时间为129天。两组之间在人口统计学或合并症变量方面无基线差异(P > 0.05)。杂交组手术时间较短(255分钟对306分钟;P = 0.01),术后住院时间较短(10.1天对13.3天;P = 0.02),且开放手术时失血量减少(1300毫升对2600毫升;P = 0.01)。尽管杂交组急性肾损伤发生率较高(76.0%对51.1%;P = 0.03),但肾衰竭发生率无差异(8.0%对4.5%;P = 0.84)。分期杂交组MAE发生率较低(20.0%对48.9%;P = 0.01),住院死亡率无差异(4.0%对3.4%;P = 0.89)。杂交组中位总成本较高(112,920美元对72,037美元;P = 0.003)。使用平均成本时,杂交组价值提高了56%,使用中位成本时提高了178%。
与开放性修复术相比,II型TAAA分期杂交修复术相关的20%的MAE发生率显著降低,相对降低超过50%。尽管医院总成本较高,但与标准开放性修复术相比,分期杂交修复术的医疗保健相关价值高56%至178%。在日益关注成本和质量的时代背景下,广泛TAAA的分期杂交修复术与开放性TAAA修复术相比并发症更少,从资源利用角度来看是一项具有良好价值的投资。