Brinkman William B, Lipstein Ellen A, Taylor Janalee, Schoettker Pamela J, Naylor Katherine, Jones Karla, Vora Sheetal S, Mims Catherine C, Roth-Wojcicki Elizabeth, Gottlieb Beth, Griffin Nancy, Lannon Carole, Morgan Esi
Department of Pediatrics, Cincinnati Children's Hospital Medical Center, 3333 Burnet Avenue, Cincinnati, OH, 45229, USA.
University of Cincinnati College of Design, Architecture, Art and Planning, 5470 Aronoff, Cincinnati, OH, 45221, USA.
Pediatr Rheumatol Online J. 2017 Jun 5;15(1):48. doi: 10.1186/s12969-017-0177-x.
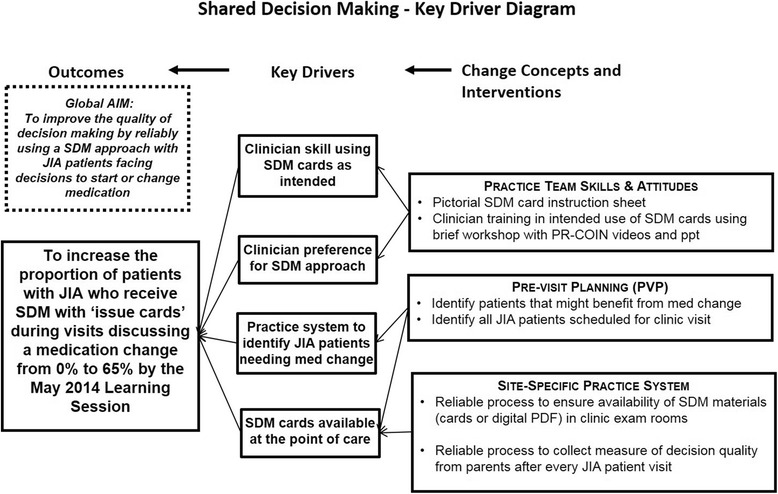
Randomized trials have demonstrated the efficacy of patient decision aids to facilitate shared decision making in clinical situations with multiple medically reasonable options for treatment. However, little is known about how best to implement these tools into routine clinical practice. In addition, reliable implementation of decision aids has been elusive and spread within pediatrics has been slow. We sought to develop and reliably implement a decision aid for treatment of children with juvenile idiopathic arthritis.
To design our decision aid, we partnered with patient, parent, and clinician stakeholders from the Pediatric Rheumatology Care and Outcomes Improvement Network. Six sites volunteered to use quality improvement methods to implement the decision aid. Four of these sites collected parent surveys following visits to assess outcomes. Parents reported on clinician use of the decision aid and the amount of shared decision making and uncertainty they experienced. We used chi-square tests to compare eligible visits with and without use of the decision aid on the experience of shared decision making and uncertainty.
After 18 rounds of testing and revision, stakeholders approved the decision aid design for regular use. Qualitative feedback from end-users was positive. During the implementation project, the decision aid was used in 35% of visits where starting or switching medication was discussed. Clinicians used the decision aid as intended in 68% of these visits. The vast majority of parents reported high levels of shared decision making following visits with (64/76 = 84%) and without (80/95 = 84%) use of the decision aid (p = 1). Similarly, the vast majority of parents reported no uncertainty following visits with (74/76 = 97%) and without (91/95 = 96%) use of the decision aid (p = 0.58).
Although user acceptability of the decision aid was high, reliable implementation in routine clinical care proved challenging. Our parsimonious approach to outcome assessment failed to detect a difference between visits with and without use of our aid. Innovative approaches are needed to facilitate use of decision aids and the assessment of outcomes.
随机试验已证明患者决策辅助工具在临床存在多种合理治疗选择的情况下促进共同决策的有效性。然而,对于如何最好地将这些工具应用于常规临床实践知之甚少。此外,决策辅助工具的可靠实施一直难以实现,在儿科领域的推广也很缓慢。我们试图开发并可靠实施一种针对幼年特发性关节炎患儿治疗的决策辅助工具。
为设计我们的决策辅助工具,我们与儿科风湿病护理与结局改善网络的患者、家长和临床医生利益相关者合作。六个地点自愿采用质量改进方法来实施该决策辅助工具。其中四个地点在就诊后收集家长调查问卷以评估结局。家长报告临床医生对决策辅助工具的使用情况以及他们经历的共同决策程度和不确定性。我们使用卡方检验来比较使用和未使用决策辅助工具的合格就诊在共同决策体验和不确定性方面的差异。
经过18轮测试和修订,利益相关者批准了决策辅助工具的设计以供常规使用。终端用户的定性反馈是积极的。在实施项目期间,在讨论开始或更换药物的就诊中,35%使用了该决策辅助工具。在这些就诊中,68%的临床医生按预期使用了决策辅助工具。绝大多数家长报告在使用(64/76 = 84%)和未使用(80/95 = 84%)决策辅助工具的就诊后共同决策程度较高(p = 1)。同样,绝大多数家长报告在使用(74/76 = 97%)和未使用(91/95 = 96%)决策辅助工具的就诊后没有不确定性(p = 0.58)。
尽管决策辅助工具的用户接受度很高,但在常规临床护理中的可靠实施证明具有挑战性。我们对结局评估的简约方法未能检测出使用和未使用我们的辅助工具的就诊之间的差异。需要创新方法来促进决策辅助工具的使用和结局评估。