Akmatov Manas K, Röber Nadja, Ahrens Wolfgang, Flesch-Janys Dieter, Fricke Julia, Greiser Halina, Günther Kathrin, Kaaks Rudolf, Kemmling Yvonne, Krone Bastian, Linseisen Jakob, Meisinger Christa, Moebus Susanne, Obi Nadia, Guzman Carlos A, Conrad Karsten, Pessler Frank
TWINCORE, Centre for Experimental and Clinical Infection Research, Feodor-Lynen-Straße 7, 30625, Hannover, Germany.
Helmholtz Centre for Infection Research, Braunschweig, Germany.
Arthritis Res Ther. 2017 Jun 6;19(1):127. doi: 10.1186/s13075-017-1338-5.
We determined the prevalence of anti-nuclear autoantibodies (ANAs) in the German adult population and examined the association between ANAs and cardiovascular and metabolic disorders.
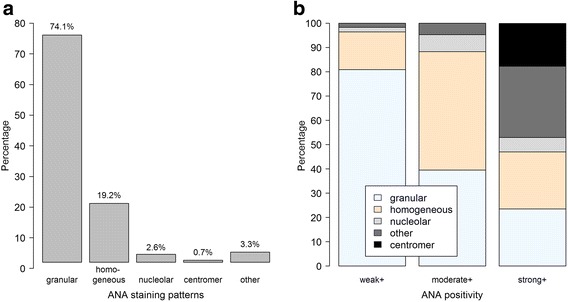
We used data and blood samples from the pretest phases of the German National Cohort, obtained from six of the 18 study centers (n = 1199). All centers applied standardized instruments including face-to-face interviews, anthropometric measurements and collection of blood samples. Self-reported histories of diabetes mellitus, heart attack and elevated blood cholesterol and/or lipids were recorded. Height, weight and blood pressure were measured. ANAs were detected using a semi-automated system (AKLIDES®; Medipan GmbH, Dahlewitz, Germany). A positive ANA was defined as a titer ≥ 1:80. ANA were classified as weakly (1:80 or 1:160), moderately (1:320 or 1:640) or strongly (≥1:1280) positive. Specific autoantibodies against nuclear antigens were detected with second-step assays according to the ANA staining pattern. Associations between the assessed disorders and ANA positivity and pattern were examined using sex and age-adjusted mixed-effects logistic regression models.
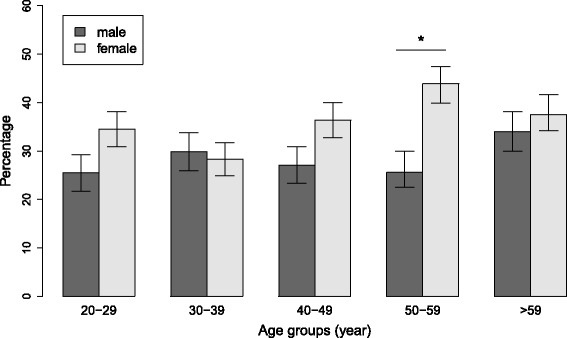
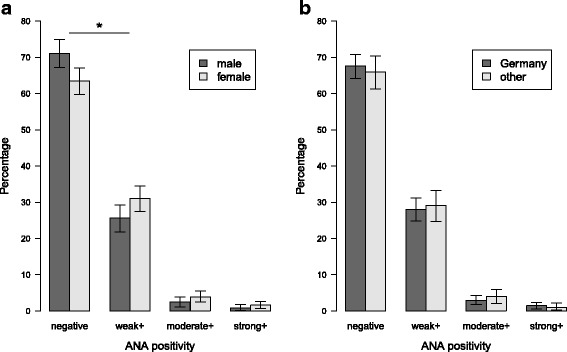
Thirty-three percent (95% confidence interval; 31-36%) of the 1196 participants (measurements could not be obtained from three samples) were ANA positive (titer ≥ 1:80). The proportions of weakly, moderately and strongly positive ANA were 29%, 3.3% and 1.3%, respectively. ANA positivity was more common among women than men across all titers (χ, p = 0.03). ANA positivity, even when stratified according to height of titer or immunofluorescent pattern, was not associated with diabetes, elevated blood cholesterol and/or lipids, obesity or hypertension. Second-step autoantibody assays were positive in 41 of the 83 samples (49%) tested, with anti-DFS70 (n = 13) and anti-dsDNA (n = 7) being most frequent. These subgroups were too small to test for associations with the disorders assessed.
The prevalence of ANA positivity in the German general population was similar to values reported from other countries. Contrary to other studies, there was no association with selected self-reported and objectively measured cardiovascular and metabolic variables.
我们确定了德国成年人群中抗核自身抗体(ANA)的患病率,并研究了ANA与心血管和代谢紊乱之间的关联。
我们使用了来自德国国民队列预测试阶段的数据和血样,这些数据和血样来自18个研究中心中的6个(n = 1199)。所有中心都采用了标准化工具,包括面对面访谈、人体测量和血样采集。记录了自我报告的糖尿病、心脏病发作以及血胆固醇和/或血脂升高的病史。测量了身高、体重和血压。使用半自动系统(AKLIDES®;德国达勒维茨的Medipan GmbH公司)检测ANA。ANA阳性定义为滴度≥1:80。ANA被分类为弱阳性(1:80或1:160)、中度阳性(1:320或1:640)或强阳性(≥1:1280)。根据ANA染色模式,通过第二步检测法检测针对核抗原的特异性自身抗体。使用性别和年龄调整的混合效应逻辑回归模型检查评估的疾病与ANA阳性及模式之间的关联。
1196名参与者(无法从三个样本中获得测量值)中有33%(95%置信区间;31 - 36%)ANA呈阳性(滴度≥1:80)。弱阳性、中度阳性和强阳性ANA的比例分别为29%、3.3%和1.3%。在所有滴度水平上,女性中ANA阳性比男性更常见(χ²,p = 0.03)。即使根据滴度高度或免疫荧光模式进行分层,ANA阳性也与糖尿病、血胆固醇和/或血脂升高、肥胖或高血压无关。在83个检测样本中的41个(49%)中,第二步自身抗体检测呈阳性,其中抗DFS70(n = 13)和抗双链DNA(n = 7)最为常见。这些亚组规模太小,无法检测与所评估疾病的关联。
德国普通人群中ANA阳性的患病率与其他国家报告的值相似。与其他研究相反,ANA与选定的自我报告和客观测量的心血管及代谢变量之间没有关联。