van der Kooy Jacoba, Birnie Erwin, Denktas Semiha, Steegers Eric A P, Bonsel Gouke J
Department of Obstetrics and Gynecology, Division of Obstetrics & Prenatal Medicine, Room Hs-408, Erasmus MC, PO Box 2040, 3000, CA, Rotterdam, The Netherlands.
Institute of Health Policy and Management, Erasmus University Rotterdam, PO Box 1738, 3000, DR, Rotterdam, The Netherlands.
BMC Pregnancy Childbirth. 2017 Jun 8;17(1):177. doi: 10.1186/s12884-017-1348-y.
To compare the mode of delivery between planned home versus planned hospital births and to determine if differences in intervention rates could be interpreted as over- or undertreatment.
Intervention and perinatal mortality rates were obtained for 679,952 low-risk women from the Dutch Perinatal Registry (2000-2007). Intervention was defined as operative vaginal delivery and/or caesarean section. Perinatal mortality was defined as the intrapartum and early neonatal mortality rate up to 7 days postpartum. Besides adjustment for maternal and care factors, we included for additional casemix adjustment: presence of congenital abnormality, small for gestational age, preterm birth, or low Apgar score. The techniques used were nested multiple stepwise logistic regression, and stratified analysis for separate risk groups. An intention-to-treat like analysis was performed.
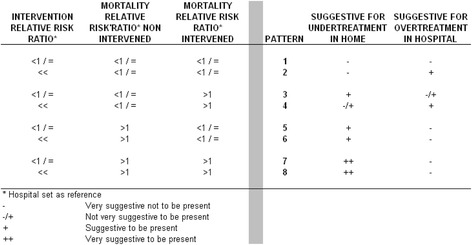
The intervention rate was lower in planned home compared to planned hospital births (10.9% 95% CI 10.8-11.0 vs. 13.8% 95% CI 13.6-13.9). Intended place of birth had significant impact on the likelihood to intervene after adjustment (planned homebirth (OR 0.77 95% CI. 0.75-0.78)). The mortality rate was lower in planned home births (0.15% vs. 0.18%). After adjustment, the interaction term home- intervention was significant (OR1.51 95% CI 1.25-1.84). In risk groups, a higher perinatal mortality rate was observed in planned home births.
The potential presence of over- or under treatment as expressed by adjusted perinatal mortality differs per risk group. In planned home births especially multiparous women showed universally lower intervention rates. However, the benefit of substantially fewer interventions in the planned home group seems to be counterbalanced by substantially increased mortality if intervention occurs.
比较计划在家分娩与计划在医院分娩的分娩方式,并确定干预率的差异是否可解释为过度治疗或治疗不足。
从荷兰围产期登记处(2000 - 2007年)获取了679952名低风险女性的干预率和围产期死亡率。干预定义为手术阴道分娩和/或剖宫产。围产期死亡率定义为分娩期和产后7天内的早期新生儿死亡率。除了对母亲和护理因素进行调整外,我们还进行了额外的病例组合调整:是否存在先天性异常、小于胎龄、早产或阿氏评分低。所使用的技术是嵌套多重逐步逻辑回归,以及对不同风险组的分层分析。进行了意向性治疗类分析。
与计划在医院分娩相比,计划在家分娩的干预率较低(10.9%,95%可信区间10.8 - 11.0 vs. 13.8%,95%可信区间13.6 - 13.9)。调整后,预期分娩地点对干预可能性有显著影响(计划在家分娩(比值比0.77,95%可信区间0.75 - 0.78))。计划在家分娩的死亡率较低(0.15%对0.18%)。调整后,家庭 - 干预交互项显著(比值比1.51,95%可信区间1.25 - 1.84)。在风险组中,计划在家分娩的围产期死亡率较高。
根据调整后的围产期死亡率表示的过度治疗或治疗不足的潜在情况因风险组而异。在计划在家分娩中,尤其是经产妇的干预率普遍较低。然而,如果进行干预,计划在家分娩组中干预大幅减少的益处似乎被死亡率大幅增加所抵消。