Camacho Fabian T, Tan Xi, Alcalá Héctor E, Shah Surbhi, Anderson Roger T, Balkrishnan Rajesh
Department of Public Health Science, University of Virginia School of Medicine West Virginia, School of Pharmacy, Charlottesville, VA University of Georgia, College of Pharmacy, Athens, GA.
Medicine (Baltimore). 2017 Jun;96(24):e7147. doi: 10.1097/MD.0000000000007147.
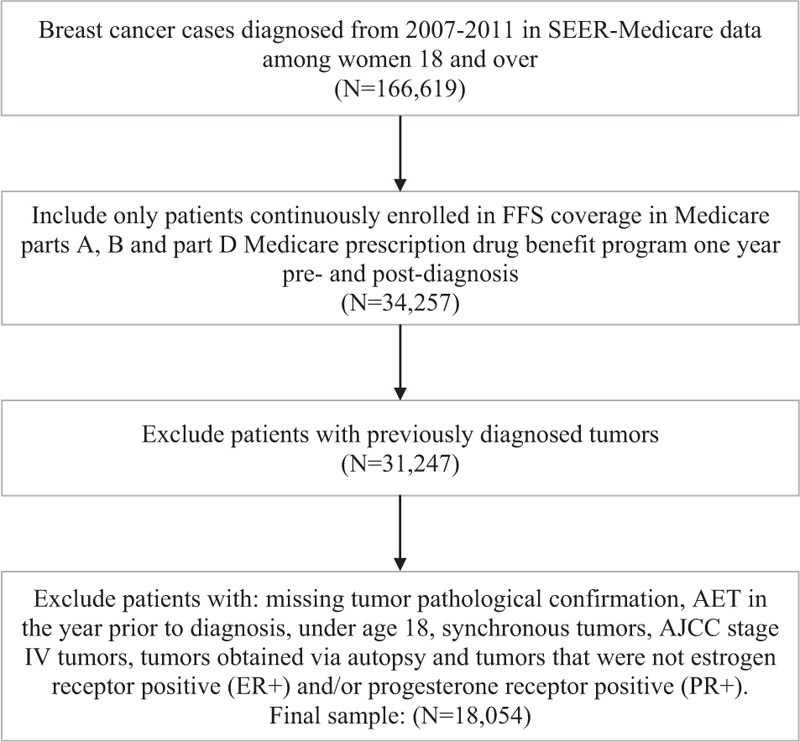
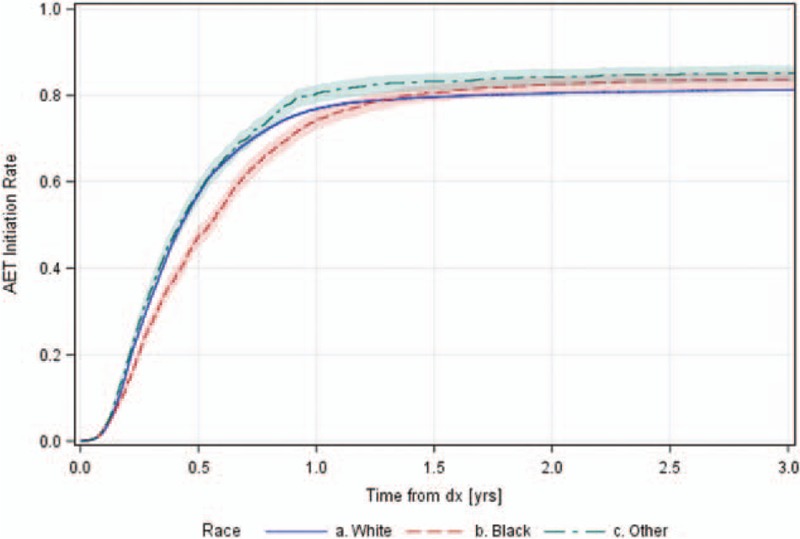
To evaluate variations in the use of adjuvant endocrine therapy (AET) by race and geography, this research examined their influence on initiation and adherence to AET in female Medicare enrollees with breast cancer, diagnosed between 2007 and 2011.Using SEER (Surveillance, Epidemiology, and End Results Program)-Medicare data from 2007 to 2001, logistic regressions with random intercept for county of residence were used to predict AET initiation during 1st year and AET adherence assessed by the medication possession ratio (MPR) during year after initiation in a sample of fee-for-service medicare beneficiaries. Part D enrollment was required for the examination of adherence. Independent variables examined were race (black, white, or other) and geographical indicators (area deprivation, non-metropolitan status, and physician shortage).Overall, 23% of patients did not initiate AET within 1 year and 26% of the initiation sample was not adherent to AET, with average follow-up time among initiators of 141 days and an average MPR of 0.84. Significant heterogeneity (P < .01) was found between SEER sites, with initiation rates as low as 69% for Washington and as high as 81% for New Jersey; MPR adherence varied from 77% in New Jersey to 68% in Utah.Blacks had lower initiation, enrollees not in Medicaid had lower adherence, lower area deprivation counties had lower initiation, earlier SEER-Medicare years had both later initiation and nonadherence, and significant (P < .05) variations between SEER sites remained after accounting for area deprivation index, metropolitan status, and physician shortage. Subgroup analysis showed particular pockets of lower initiation for blacks with stage III tumors, on chemotherapy and lower adherence for blacks in youngest age group, with stage III tumors, tamoxifen use and blacks/others in oldest age group.Black women and women living in states with more rurality in the United States were less likely to receive guideline-recommended AET, which necessitates future efforts to alleviate these disparities to improve AET use and ultimately pursue more survival gains through optimizing adjuvant treatment use among cancer survivors.
为评估种族和地域因素对辅助内分泌治疗(AET)使用情况的影响,本研究调查了2007年至2011年间确诊为乳腺癌的女性医疗保险参保者中,种族和地域因素对AET起始治疗及治疗依从性的影响。利用2007年至2011年的监测、流行病学及最终结果(SEER)计划 - 医疗保险数据,对按服务收费的医疗保险受益人的样本,采用带有居住县随机截距的逻辑回归模型,预测第1年的AET起始治疗情况,并通过起始治疗后1年的药物持有率(MPR)评估AET依从性。检查依从性时需要参保D部分。所检查的自变量为种族(黑人、白人或其他)和地理指标(地区贫困程度、非都市状态和医生短缺情况)。总体而言,23%的患者在1年内未开始AET治疗,起始治疗的患者中有26%未坚持AET治疗,起始治疗患者的平均随访时间为141天,平均MPR为0.84。在SEER各地区之间发现了显著的异质性(P<0.01),华盛顿的起始治疗率低至69%,新泽西高达81%;MPR依从性从新泽西的77%到犹他州的68%不等。黑人的起始治疗率较低,非医疗补助参保者的依从性较低,贫困程度较低的县起始治疗率较低,SEER - 医疗保险数据较早期的年份起始治疗和不依从情况都较晚,并且在考虑地区贫困指数、都市状态和医生短缺情况后,SEER各地区之间仍存在显著(P<0.05)差异。亚组分析显示,患有III期肿瘤、正在接受化疗的黑人起始治疗率较低,最年轻年龄组中患有III期肿瘤、使用他莫昔芬的黑人以及最年长年龄组中的黑人/其他种族的人依从性较低。美国的黑人女性以及居住在农村地区较多的州的女性接受指南推荐的AET治疗的可能性较小,这就需要未来做出努力来缓解这些差异,以改善AET的使用情况,并最终通过优化癌症幸存者的辅助治疗使用来获得更多的生存收益。