Marenghi Cristina, Alvisi Maria Francesca, Palorini Federica, Avuzzi Barbara, Badenchini Fabio, Bedini Nice, Bellardita Lara, Biasoni Davide, Bosetti Davide, Casale Alessandra, Catanzaro Mario, Colecchia Maurizio, De Luca Letizia, Donegani Simona, Dordoni Paola, Lanocita Rodolfo, Maffezzini Massimo, Magnani Tiziana, Menichetti Julia, Messina Antonella, Morlino Sara, Paolini Biagio, Rancati Tiziana, Stagni Silvia, Tesone Antonio, Torelli Tullio, Tulli Baldoin Edoardo, Vaiani Marta, Villa Sergio, Villa Silvia, Zaffaroni Nadia, Nicolai Nicola, Salvioni Roberto, Valdagni Riccardo
Prostate Cancer Program, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan - Italy.
Division of Radiation Oncology 1, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan - Italy.
Tumori. 2017 Sep 18;103(5):464-474. doi: 10.5301/tj.5000649. Epub 2017 Jun 14.
To evaluate the outcomes of active surveillance (AS) on patients with low-risk prostate cancer (PCa) and to identify predictors of disease reclassification.
In 2005, we defined an institutional AS protocol (Sorveglianza Attiva Istituto Nazionale Tumori [SAINT]), and we joined the Prostate Cancer Research International: Active Surveillance (PRIAS) study in 2007. Eligibility criteria included clinical stage ≤T2a, initial prostate-specific antigen (PSA) <10 ng/mL, and Gleason Pattern Score (GPS) ≤3 + 3 (both protocols); ≤25% positive cores with a maximum core length containing cancer ≤50% (SAINT); and ≤2 positive cores and PSA density <0.2 ng/mL/cm3 (PRIAS). Switching to active treatment was advised for a worsening of GPS, increased positive cores, or PSA doubling time <3 years. Active treatment-free survival (ATFS) was assessed using the Kaplan-Meier method. Factors associated with ATFS were evaluated with a multivariate Cox proportional hazards model.
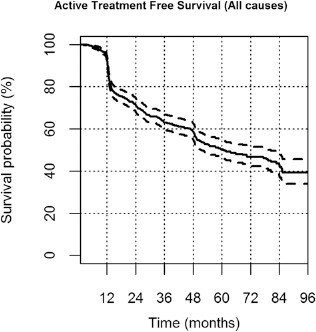
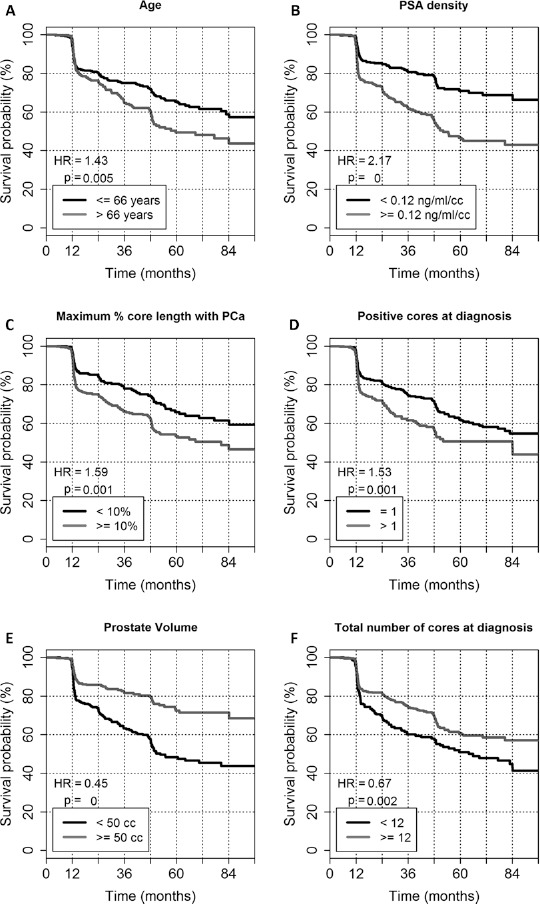
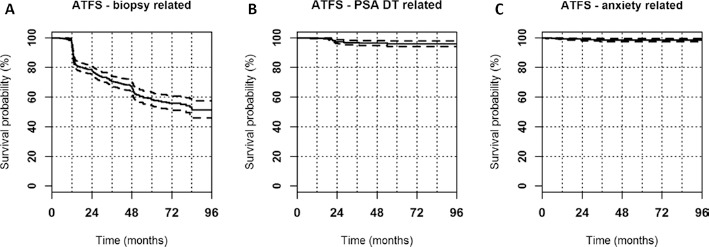
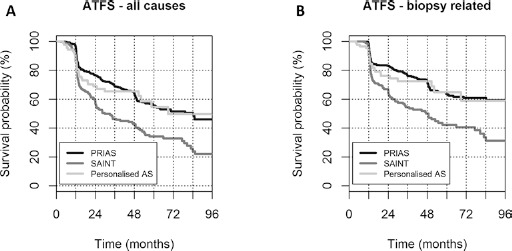
A total of 818 patients were included: 200 in SAINT, 530 in PRIAS, and 88 in personalized AS monitoring. Active treatment-free survival was 50% after a median follow-up of 60 months. A total of 404/818 patients (49.4%) discontinued AS: 274 for biopsy-related reclassification, 121/404 (30%) for off-protocol reasons, 9/404 (2.2%) because of anxiety. Biopsy reclassification was associated with PSA density (hazard ratio [HR] 1.8), maximum percentage of core involvement (HR 1.5), positive cores at diagnostic biopsy (HR 1.6), older age (HR 1.5), and prostate volume (HR 0.6) (all p<0.01). Patients from SAINT were significantly more likely to discontinue AS than were the patients from PRIAS (HR 1.65, p<0.0001).
Five years after diagnosis, 50% of patients with early PCa were spared from active treatment. Wide inclusion criteria are associated with lower ATFS. However, at preliminary analysis, this does not seem to affect the probability of unfavorable pathology.
评估主动监测(AS)对低风险前列腺癌(PCa)患者的疗效,并确定疾病重新分类的预测因素。
2005年,我们制定了一项机构性AS方案(国立肿瘤研究所主动监测[SAINT]),并于2007年加入了国际前列腺癌研究:主动监测(PRIAS)研究。纳入标准包括临床分期≤T2a、初始前列腺特异性抗原(PSA)<10 ng/mL以及Gleason模式评分(GPS)≤3+3(两项方案);阳性核心≤25%,含癌的最大核心长度≤50%(SAINT);以及阳性核心≤2个且PSA密度<0.2 ng/mL/cm³(PRIAS)。若GPS恶化、阳性核心增加或PSA倍增时间<3年,则建议转为积极治疗。采用Kaplan-Meier法评估无积极治疗生存期(ATFS)。使用多变量Cox比例风险模型评估与ATFS相关的因素。
共纳入818例患者:SAINT组200例,PRIAS组530例,个性化AS监测组88例。中位随访60个月后,无积极治疗生存期为50%。共有404/818例患者(49.4%)停止AS:274例因活检相关重新分类,121/404例(30%)因不符合方案标准的原因,9/404例(2.2%)因焦虑。活检重新分类与PSA密度(风险比[HR] 1.8)、核心受累的最大百分比(HR 1.5)、诊断性活检时的阳性核心(HR 1.6)、年龄较大(HR 1.5)以及前列腺体积(HR )相关(均p<0.01)。SAINT组的患者比PRIAS组的患者更有可能停止AS(HR 1.65,p<0.0001)。
诊断后5年,50%的早期PCa患者无需接受积极治疗。广泛的纳入标准与较低的ATFS相关。然而,在初步分析中,这似乎并不影响不良病理的概率。