Elovainio Marko, Hakulinen Christian, Pulkki-Råback Laura, Virtanen Marianna, Josefsson Kim, Jokela Markus, Vahtera Jussi, Kivimäki Mika
Department of Psychology and Logopedics, Faculty of Medicine, University of Helsinki, Helsinki, Finland; Department of Health Services Research, National Institute for Health and Welfare, Helsinki, Finland.
Department of Psychology and Logopedics, Faculty of Medicine, University of Helsinki, Helsinki, Finland; Department of Health Services Research, National Institute for Health and Welfare, Helsinki, Finland.
Lancet Public Health. 2017 May 4;2(6):e260-e266. doi: 10.1016/S2468-2667(17)30075-0. eCollection 2017 Jun.
The associations of social isolation and loneliness with premature mortality are well known, but the risk factors linking them remain unclear. We sought to identify risk factors that might explain the increased mortality in socially isolated and lonely individuals.
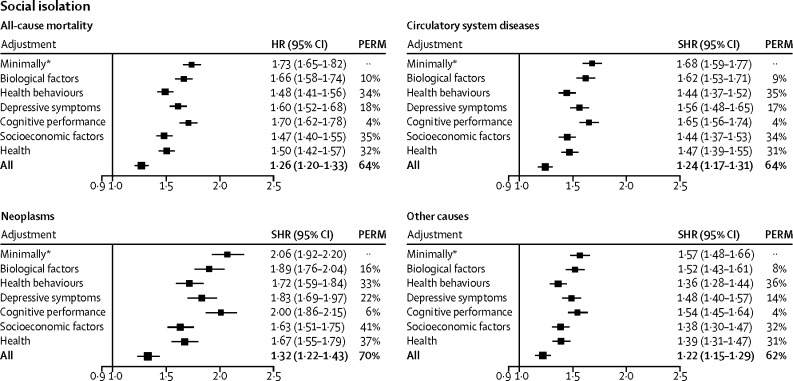
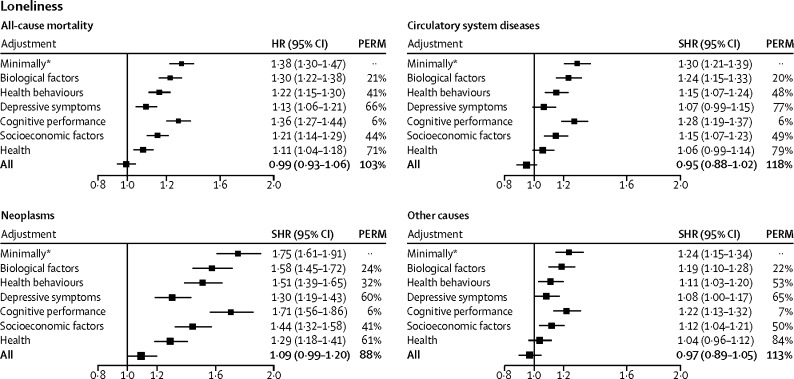
We used prospective follow-up data from the UK Biobank cohort study to assess self-reported isolation (a three-item scale) and loneliness (two questions). The main outcomes were all-cause and cause-specific mortality. We calculated the percentage of excess risk mediated by risk factors to assess the extent to which the associations of social isolation and loneliness with mortality were attributable to differences between isolated and lonely individuals and others in biological (body-mass index, systolic and diastolic blood pressure, and handgrip strength), behavioural (smoking, alcohol consumption, and physical activity), socioeconomic (education, neighbourhood deprivation, and household income), and psychological (depressive symptoms and cognitive capacity) risk factors.
466 901 men and women (mean age at baseline 56·5 years [SD 8·1]) were included in the analyses, with a mean follow-up of 6·5 years (SD 0·8). The hazard ratio for all-cause mortality for social isolation compared with no social isolation was 1·73 (95% CI 1·65-1·82) after adjustment for age, sex, ethnic origin, and chronic disease (ie, minimally adjusted), and was 1·26 (95% CI 1·20-1·33) after further adjustment for socioeconomic factors, health-related behaviours, depressive symptoms, biological factors, cognitive performance, and self-rated health (ie, fully adjusted). The minimally adjusted hazard ratio for mortality risk related to loneliness was 1·38 (95% CI 1·30-1·47), which reduced to 0·99 (95% CI 0·93-1·06) after full adjustment for baseline risks.
Isolated and lonely people are at increased risk of death. Health policies addressing risk factors such as adverse socioeconomic conditions, unhealthy lifestyle, and lower mental wellbeing might reduce excess mortality among the isolated and the lonely.
Academy of Finland, NordForsk, and the UK Medical Research Council.
社会孤立和孤独与过早死亡之间的关联已广为人知,但将它们联系起来的风险因素仍不明确。我们试图确定可能解释社会孤立和孤独个体死亡率增加的风险因素。
我们使用英国生物银行队列研究的前瞻性随访数据来评估自我报告的孤立感(一个包含三个项目的量表)和孤独感(两个问题)。主要结局是全因死亡率和特定原因死亡率。我们计算了由风险因素介导的额外风险百分比,以评估社会孤立和孤独与死亡率之间的关联在多大程度上可归因于孤立和孤独个体与其他人在生物学(体重指数、收缩压和舒张压以及握力)、行为(吸烟、饮酒和身体活动)、社会经济(教育、邻里贫困和家庭收入)以及心理(抑郁症状和认知能力)风险因素方面的差异。
分析纳入了466901名男性和女性(基线时平均年龄56.5岁[标准差8.1]),平均随访6.5年(标准差0.8)。在对年龄、性别、种族和慢性病进行调整后(即最小调整),社会孤立与非社会孤立相比的全因死亡率风险比为1.73(95%置信区间1.65 - 1.82),在进一步对社会经济因素、健康相关行为、抑郁症状、生物学因素、认知表现和自我评定健康进行调整后(即完全调整),该风险比为1.26(95%置信区间1.20 - 1.33)。与孤独感相关的死亡率风险的最小调整风险比为1.38(95%置信区间1.30 - 1.47),在对基线风险进行完全调整后降至0.99(95%置信区间0.93 - 1.06)。
孤立和孤独的人死亡风险增加。针对不良社会经济状况、不健康生活方式和较低心理健康等风险因素的卫生政策可能会降低孤立和孤独人群的额外死亡率。
芬兰科学院、北欧研究理事会和英国医学研究理事会。