Neuroscience Research Center, Jane and John Justin Institute for Mind Health, Cook Children's Health Care System, Fort Worth, Texas, USA.
Department of Bioengineering, The University of Texas at Arlington, Arlington, Texas, USA.
Ann Clin Transl Neurol. 2024 Oct;11(10):2530-2547. doi: 10.1002/acn3.52156. Epub 2024 Oct 7.
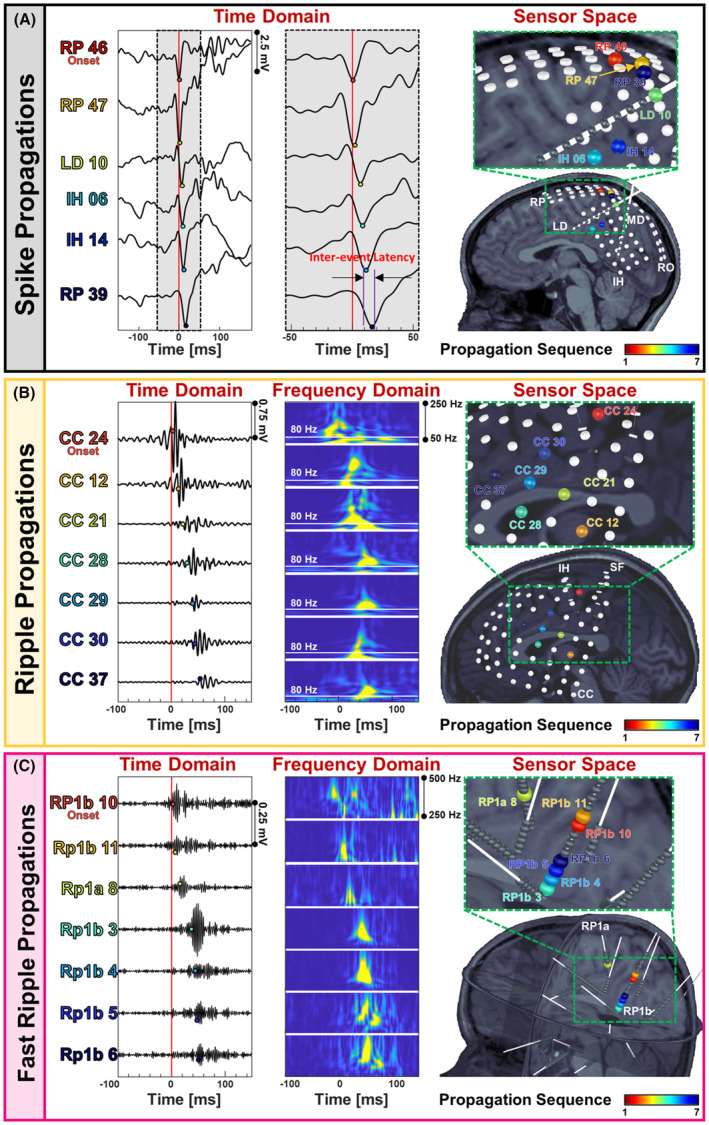
Interictal biomarkers are critical for identifying the epileptogenic focus. However, spikes and ripples lack specificity while fast ripples lack sensitivity. These biomarkers propagate from more epileptogenic onset to areas of spread. The pathophysiological mechanism of these propagations is elusive. Here, we examine zones where spikes and high frequency oscillations co-occur (SHFO), the spatiotemporal propagations of spikes, ripples, and fast ripples, and evaluate the spike-ripple onset overlap (SRO) as an epilepsy biomarker.
We retrospectively analyzed intracranial EEG data from 41 patients with drug-resistant epilepsy. We mapped propagations of spikes, ripples, and fast ripples, and identified their onset and spread zones, as well as SHFO and SRO. We then estimated the SRO prognostic value in predicting surgical outcome and compared it to onset and spread zones of spike, ripple, and fast ripple propagations, and SHFO.
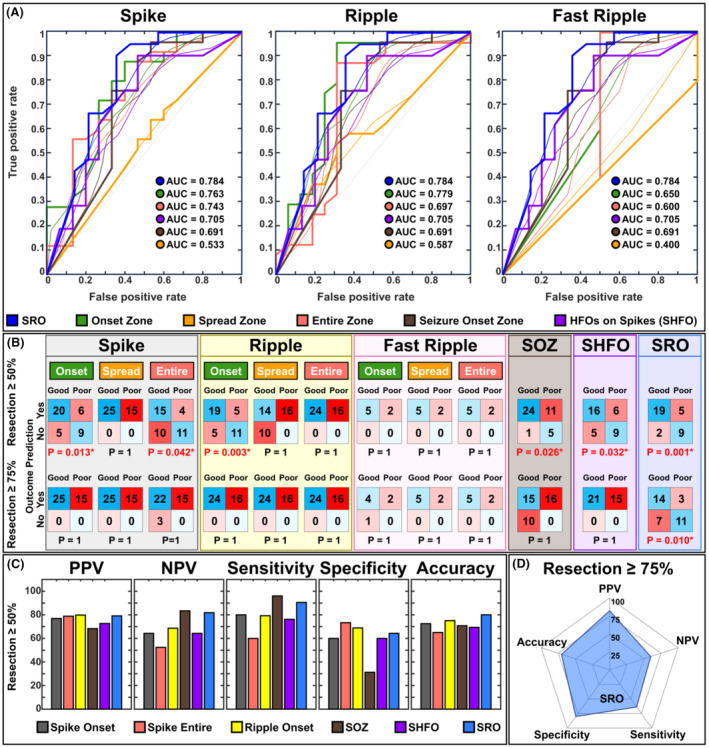
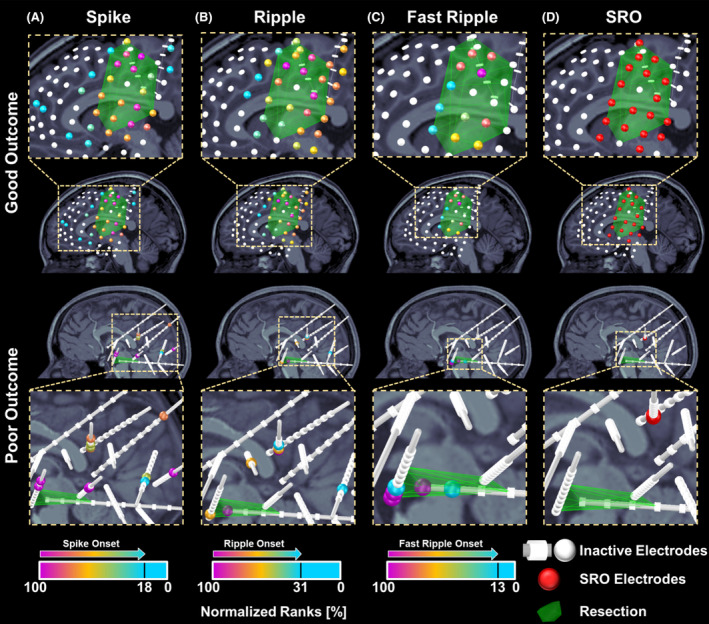
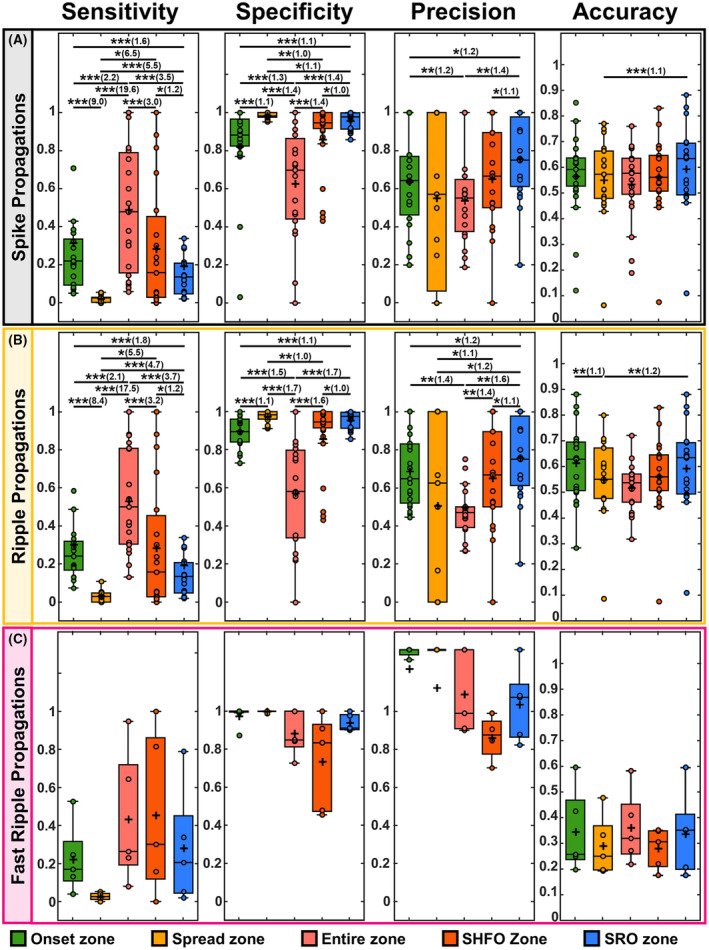
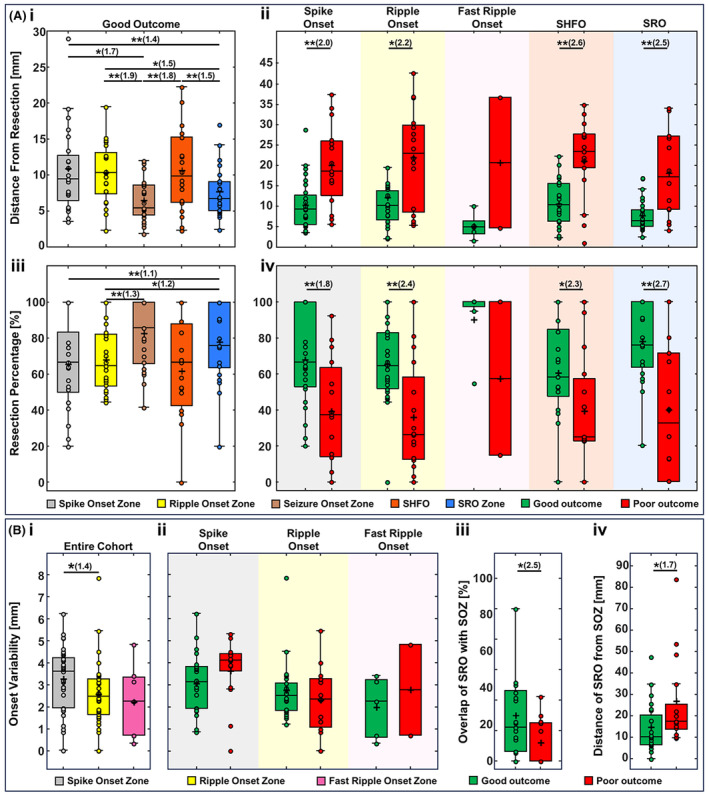
We detected spikes and ripples in all patients and fast ripples in 12 patients (29%). We observed spike and ripple propagations in 40 (98%) patients. Spike and ripple onsets overlapped in 35 (85%) patients. In good outcome patients, SRO showed higher specificity and precision (p < 0.05) in predicting resection compared to onset and zones of spikes, ripples, and SHFO. Only SRO resection predicted outcome (p = 0.01) with positive and negative predictive values of 82% and 57%, respectively.
SRO is a specific and precise biomarker of the epileptogenic zone whose removal predicts outcome. SRO is present in most patients with drug-resistant epilepsy. Such a biomarker may reduce prolonged intracranial monitoring and improve outcome.
发作间期生物标志物对于确定致痫灶至关重要。然而,棘波和涟漪缺乏特异性,而快涟漪缺乏敏感性。这些生物标志物从更具致痫性的起始部位传播到扩散区域。这些传播的病理生理机制尚不清楚。在这里,我们检查了棘波和高频振荡共同出现(SHFO)的区域,棘波、涟漪和快涟漪的时空传播,并评估了棘波-涟漪起始重叠(SRO)作为癫痫生物标志物。
我们回顾性分析了 41 例耐药性癫痫患者的颅内脑电图数据。我们绘制了棘波、涟漪和快涟漪的传播,并确定了它们的起始和传播区域,以及 SHFO 和 SRO。然后,我们估计了 SRO 在预测手术结果中的预后价值,并将其与棘波、涟漪和快涟漪传播的起始和传播区域以及 SHFO 进行了比较。
我们在所有患者中均检测到棘波和涟漪,在 12 例患者(29%)中检测到快涟漪。我们在 40 例(98%)患者中观察到棘波和涟漪的传播。在 35 例(85%)患者中,棘波和涟漪的起始重叠。在预后良好的患者中,SRO 在预测切除方面比棘波、涟漪和 SHFO 的起始和区域具有更高的特异性和精度(p<0.05)。只有 SRO 切除预测了结果(p=0.01),其阳性和阴性预测值分别为 82%和 57%。
SRO 是致痫区的特异性和精确生物标志物,其切除可预测结果。SRO 存在于大多数耐药性癫痫患者中。这种生物标志物可能会减少长时间的颅内监测并改善结果。