Clark Lucy V, Pesola Francesca, Thomas Janice M, Vergara-Williamson Mario, Beynon Michelle, White Peter D
Centre for Psychiatry, Wolfson Institute of Preventive Medicine, Bart's and the London School of Medicine and Dentistry, Queen Mary University, London, UK.
Centre for Cancer Prevention, Wolfson Institute of Preventive Medicine, Bart's and the London School of Medicine and Dentistry, Queen Mary University, London, UK.
Lancet. 2017 Jul 22;390(10092):363-373. doi: 10.1016/S0140-6736(16)32589-2. Epub 2017 Jun 22.
Graded exercise therapy is an effective and safe treatment for chronic fatigue syndrome, but it is therapist intensive and availability is limited. We aimed to test the efficacy and safety of graded exercise delivered as guided self-help.
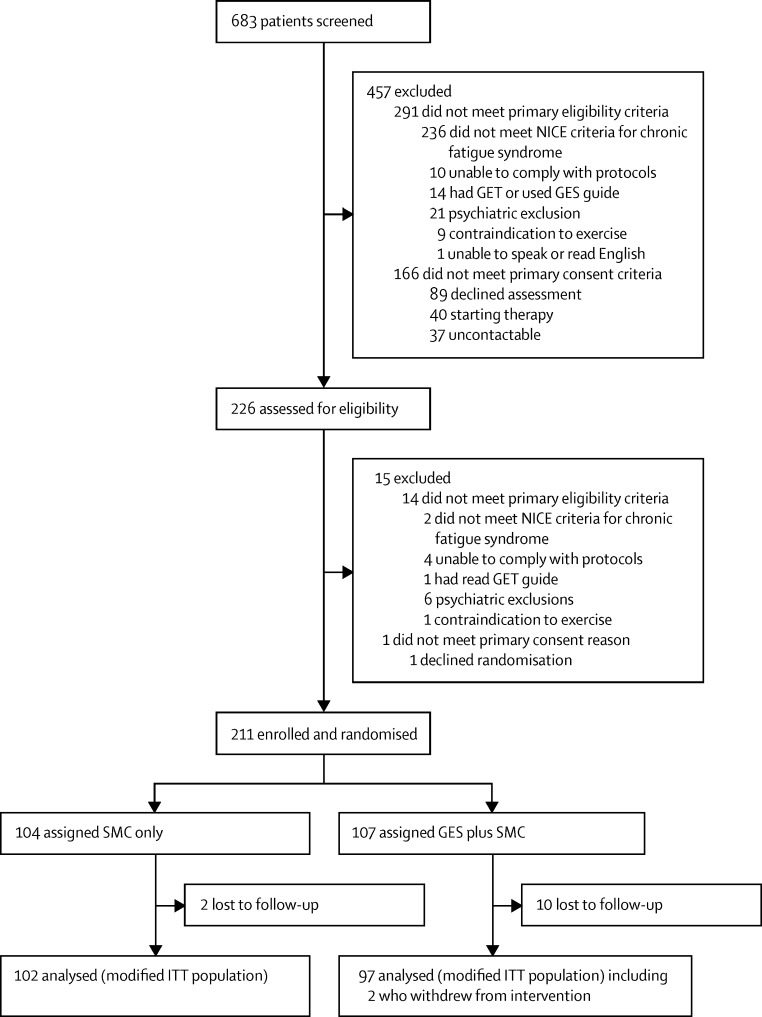
In this pragmatic randomised controlled trial, we recruited adult patients (18 years and older) who met the UK National Institute for Health and Care Excellence criteria for chronic fatigue syndrome from two secondary-care clinics in the UK. Patients were randomly assigned to receive specialist medical care (SMC) alone (control group) or SMC with additional guided graded exercise self-help (GES). Block randomisation (randomly varying block sizes) was done at the level of the individual with a computer-generated sequence and was stratified by centre, depression score, and severity of physical disability. Patients and physiotherapists were necessarily unmasked from intervention assignment; the statistician was masked from intervention assignment. SMC was delivered by specialist doctors but was not standardised; GES consisted of a self-help booklet describing a six-step graded exercise programme that would take roughly 12 weeks to complete, and up to four guidance sessions with a physiotherapist over 8 weeks (maximum 90 min in total). Primary outcomes were fatigue (measured by the Chalder Fatigue Questionnaire) and physical function (assessed by the Short Form-36 physical function subscale); both were self-rated by patients at 12 weeks after randomisation and analysed in all randomised patients with outcome data at follow-up (ie, by modified intention to treat). We recorded adverse events, including serious adverse reactions to trial interventions. We used multiple linear regression analysis to compare SMC with GES, adjusting for baseline and stratification factors. This trial is registered at ISRCTN, number ISRCTN22975026.
Between May 15, 2012, and Dec 24, 2014, we recruited 211 eligible patients, of whom 107 were assigned to the GES group and 104 to the control group. At 12 weeks, compared with the control group, mean fatigue score was 19·1 (SD 7·6) in the GES group and 22·9 (6·9) in the control group (adjusted difference -4·2 points, 95% CI -6·1 to -2·3, p<0·0001; effect size 0·53) and mean physical function score was 55·7 (23·3) in the GES group and 50·8 (25·3) in the control group (adjusted difference 6·3 points, 1·8 to 10·8, p=0·006; 0·20). No serious adverse reactions were recorded and other safety measures did not differ between the groups, after allowing for missing data.
GES is a safe intervention that might reduce fatigue and, to a lesser extent, physical disability for patients with chronic fatigue syndrome. These findings need confirmation and extension to other health-care settings.
UK National Institute for Health Research Research for Patient Benefit Programme and the Sue Estermann Fund.
分级运动疗法是治疗慢性疲劳综合征的一种有效且安全的方法,但它对治疗师的依赖程度较高,且可获得性有限。我们旨在测试以自助指导形式进行分级运动的疗效和安全性。
在这项实用随机对照试验中,我们从英国两家二级医疗诊所招募了符合英国国家卫生与临床优化研究所慢性疲劳综合征标准的成年患者(18岁及以上)。患者被随机分配接受单纯专科医疗护理(SMC)(对照组)或接受SMC并附加自助指导分级运动(GES)。在个体层面使用计算机生成的序列进行区组随机化(随机变化的区组大小),并按中心、抑郁评分和身体残疾严重程度进行分层。患者和物理治疗师必然知晓干预分配情况;统计人员对干预分配情况不知情。SMC由专科医生提供,但未标准化;GES包括一本自助手册,描述了一个分六步的分级运动计划,大约需要12周完成,以及在8周内与物理治疗师进行最多四次指导课程(总共最多90分钟)。主要结局指标为疲劳(通过查尔德疲劳问卷测量)和身体功能(通过简短健康调查问卷身体功能分量表评估);两者均由患者在随机分组后12周进行自评,并在所有有随访结局数据的随机分组患者中进行分析(即采用意向性分析的修正方法)。我们记录不良事件,包括对试验干预的严重不良反应。我们使用多元线性回归分析比较SMC和GES,并对基线和分层因素进行调整。本试验在国际标准随机对照试验编号注册库注册,编号为ISRCTN22975026。
在2012年5月15日至2014年12月24日期间,我们招募了211名符合条件患者,其中107名被分配到GES组,104名被分配到对照组。在12周时,与对照组相比,GES组的平均疲劳评分为19·1(标准差7·6),对照组为22·9(6·9)(调整后差异 -4·2分,95%置信区间 -6·1至 -2·3,p<0·0001;效应量0·53),GES组的平均身体功能评分为55·7(23·3),对照组为50·8(25·3)(调整后差异6·3分,1·8至10·8,p = 0·006;0·20)。在考虑缺失数据后,未记录到严重不良反应,且两组间其他安全指标无差异。
GES是一种安全的干预措施,可能会减轻慢性疲劳综合征患者的疲劳,并在较小程度上减轻身体残疾。这些发现需要在其他医疗环境中得到证实和扩展。
英国国家卫生研究院患者受益研究计划和苏·埃斯特曼基金。