Saito Masahide, Kadoya Noriyuki, Sato Kiyokazu, Ito Kengo, Dobashi Suguru, Takeda Ken, Onishi Hiroshi, Jingu Keiichi
Department of Radiology, University of Yamanashi, Yamanashi, Japan.
Department of Radiation Oncology, Tohoku University School of Medicine, Sendai, Japan.
J Appl Clin Med Phys. 2017 Jul;18(4):206-214. doi: 10.1002/acm2.12123. Epub 2017 Jun 26.
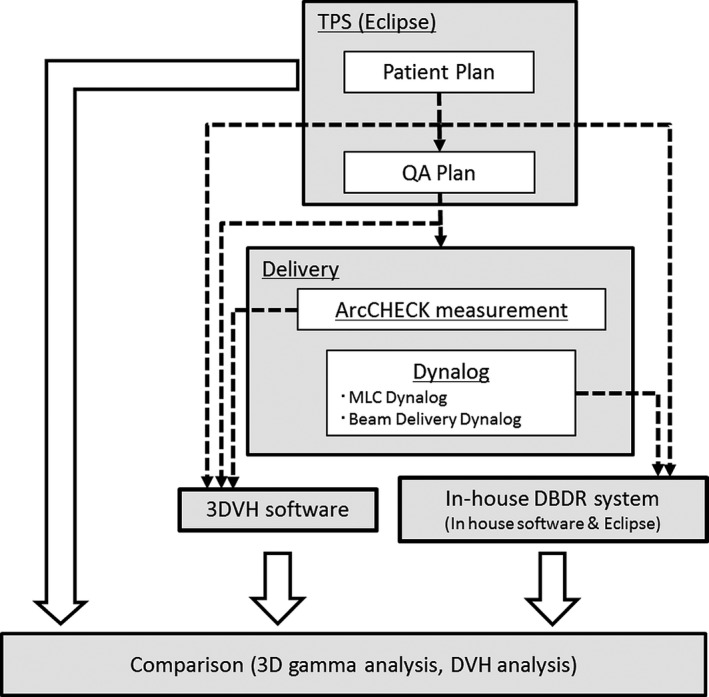
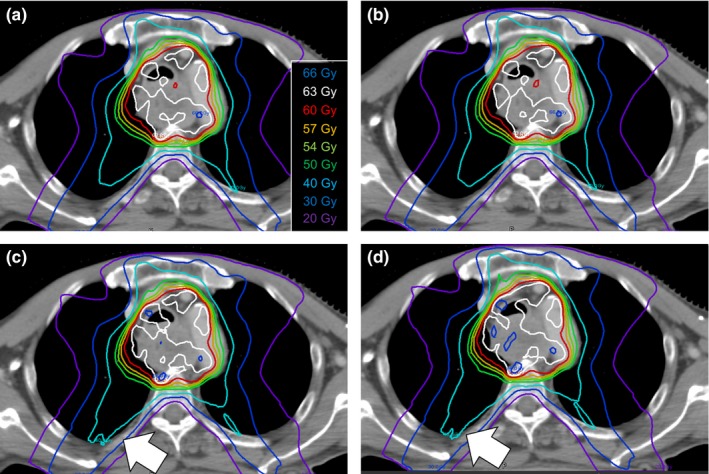
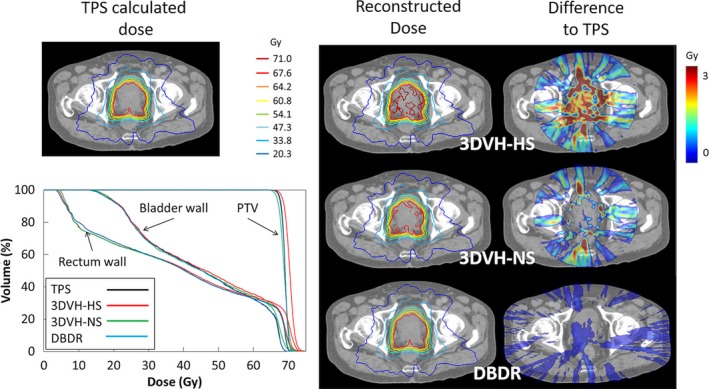
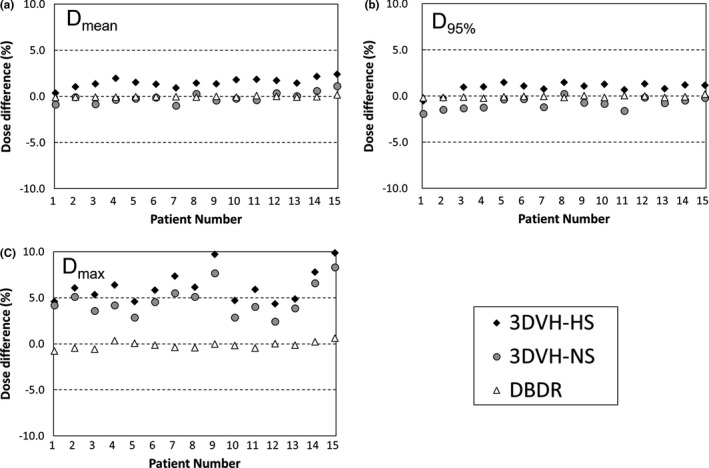
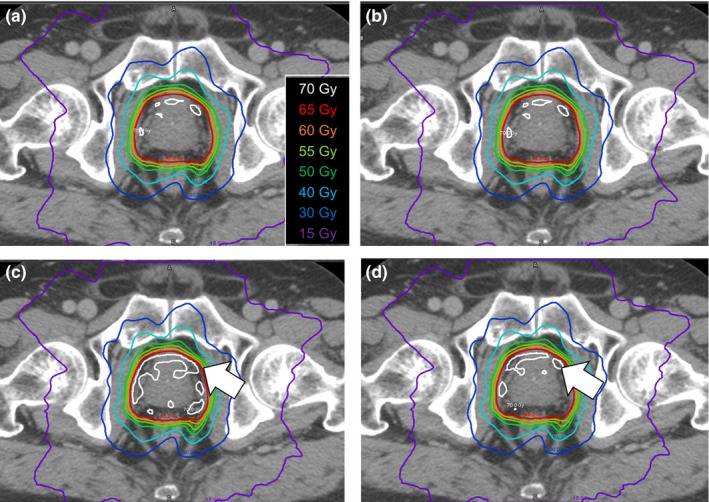
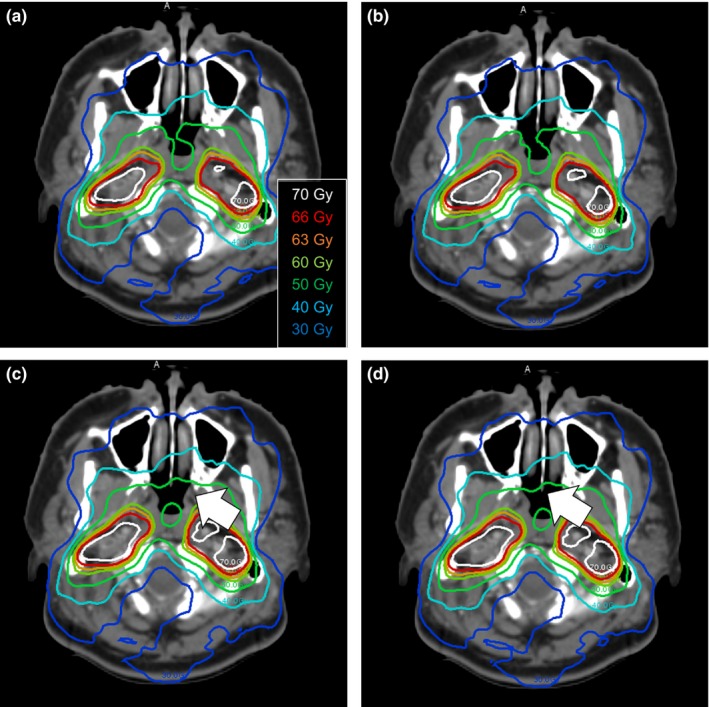
The purpose of this study was comparing dose-volume histogram (DVH)-based plan verification methods for volumetric modulated arc therapy (VMAT) pretreatment QA. We evaluated two 3D dose reconstruction systems: ArcCHECK-3DVH system (Sun Nuclear corp.) and Varian dynalog-based dose reconstruction (DBDR) system, developed in-house. Fifteen prostate cancer patients (67.6 Gy/26 Fr), four head and neck cancer patient (66 Gy/33 Fr), and four esophagus cancer patients (60 Gy/30 Fr) treated with VMAT were studied. First, ArcCHECK measurement was performed on all plans; simultaneously, the Varian dynalog data sets that contained the actual delivered parameters (leaf positions, gantry angles, and cumulative MUs) were acquired from the Linac control system. Thereafter, the delivered 3D patient dose was reconstructed by 3DVH software (two different calculating modes were used: High Sensitivity (3DVH-HS) and Normal Sensitivity (3DVH-NS)) and in-house DBDR system. We evaluated the differences between the TPS-calculated dose and the reconstructed dose using 3D gamma passing rates and DVH dose index analysis. The average 3D gamma passing rates (3%/3 mm) between the TPS-calculated dose and the reconstructed dose were 99.1 ± 0.6%, 99.7 ± 0.3%, and 100.0 ± 0.1% for 3DVH-HS, 3DVH-NS, and DBDR, respectively. For the prostate cases, the average differences between the TPS-calculated dose and reconstructed dose in the PTV mean dose were 1.52 ± 0.50%, -0.14 ± 0.55%, and -0.03 ± 0.07% for 3DVH-HS, 3DVH-NS, and DBDR, respectively. For the head and neck and esophagus cases, the dose difference to the TPS-calculated dose caused by an effect of heterogeneity was more apparent under the 3DVH dose reconstruction than the DBDR. Although with some residual dose reconstruction errors, these dose reconstruction methods can be clinically used as effective tools for DVH-based QA for VMAT delivery.
本研究的目的是比较基于剂量体积直方图(DVH)的容积调强弧形治疗(VMAT)预处理质量保证(QA)计划验证方法。我们评估了两种三维剂量重建系统:ArcCHECK-3DVH系统(太阳核公司)和内部开发的基于Varian剂量仪日志的剂量重建(DBDR)系统。研究了15例接受VMAT治疗的前列腺癌患者(67.6 Gy/26次分割)、4例头颈部癌患者(66 Gy/33次分割)和4例食管癌患者(60 Gy/30次分割)。首先,对所有计划进行ArcCHECK测量;同时,从直线加速器控制系统获取包含实际输送参数(叶片位置、机架角度和累积监测单位)的Varian剂量仪日志数据集。此后,通过3DVH软件(使用两种不同的计算模式:高灵敏度(3DVH-HS)和正常灵敏度(3DVH-NS))和内部DBDR系统重建输送的三维患者剂量。我们使用三维伽马通过率和DVH剂量指数分析评估了治疗计划系统(TPS)计算剂量与重建剂量之间的差异。对于3DVH-HS、3DVH-NS和DBDR,TPS计算剂量与重建剂量之间的平均三维伽马通过率(3%/3 mm)分别为99.1±0.6%、99.7±0.3%和100.0±0.1%。对于前列腺病例,3DVH-HS、3DVH-NS和DBDR的PTV平均剂量中TPS计算剂量与重建剂量之间的平均差异分别为1.52±0.50%、-0.14±0.55%和-0.03±0.07%。对于头颈部和食管癌病例,在3DVH剂量重建下,由不均匀性效应导致的与TPS计算剂量的剂量差异比DBDR更明显。尽管存在一些残余剂量重建误差,但这些剂量重建方法可在临床上用作基于DVH的VMAT输送QA的有效工具。