Richman Susan D, Fairley Jennifer, Butler Rachel, Deans Zandra C
Department of Pathology and Tumour Biology, Leeds Institute of Cancer and Pathology, St James University Hospital, Leeds, England, LS9 7TF, UK.
UK NEQAS for Molecular Genetics, Department of Laboratory Medicine, The Royal Infirmary, Edinburgh, Scotland, EH16 4SA, UK.
Virchows Arch. 2017 Dec;471(6):721-729. doi: 10.1007/s00428-017-2162-7. Epub 2017 Jun 26.
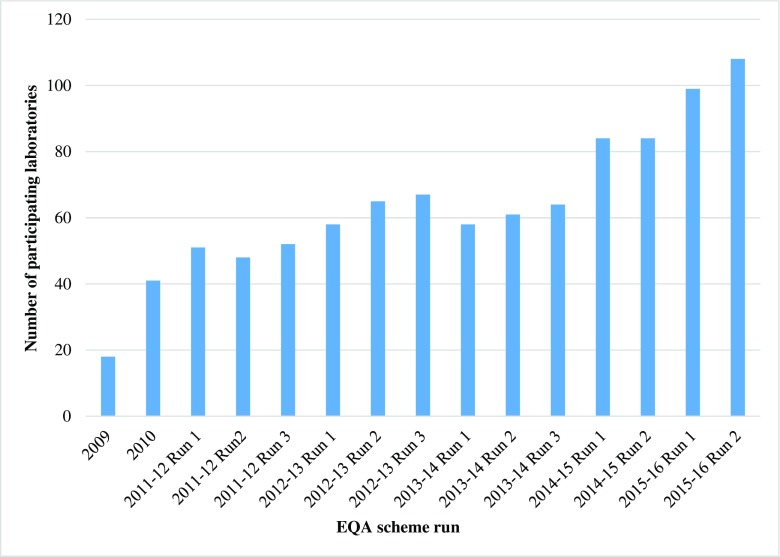
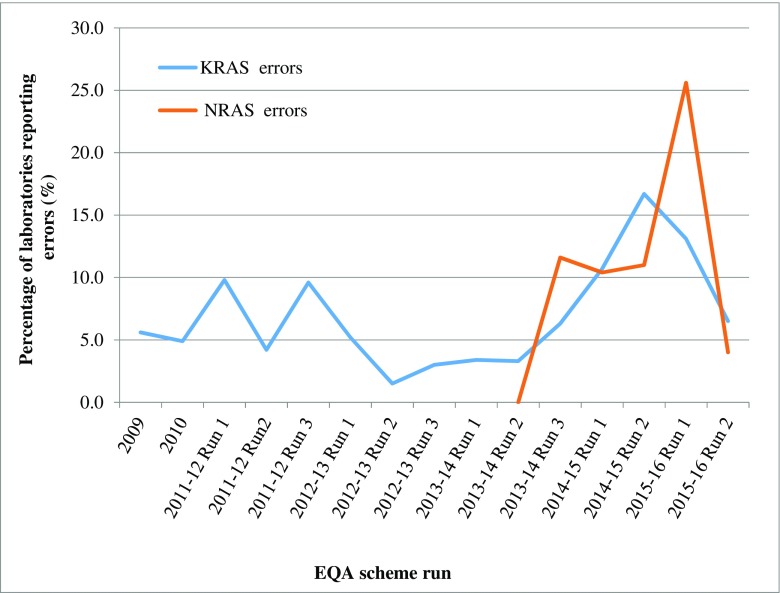
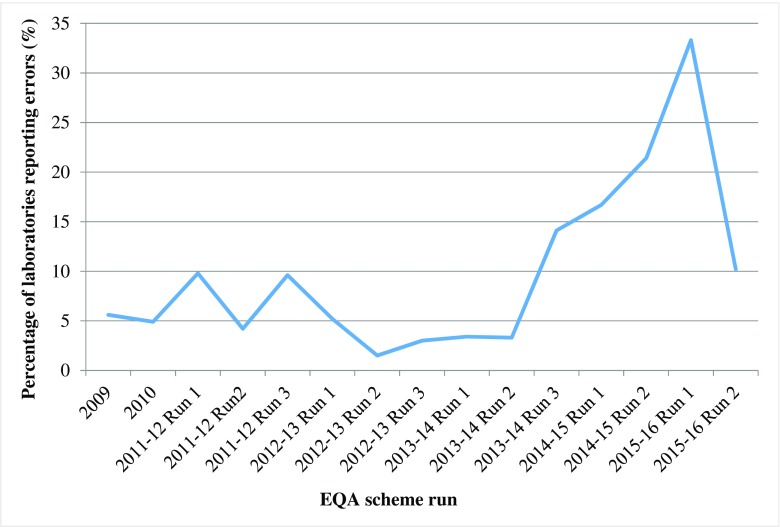
Evidence strongly indicates that extended RAS testing should be undertaken in mCRC patients, prior to prescribing anti-EGFR therapies. With more laboratories implementing testing, the requirement for External Quality Assurance schemes increases, thus ensuring high standards of molecular analysis. Data was analysed from 15 United Kingdom National External Quality Assessment Service (UK NEQAS) for Molecular Genetics Colorectal cancer external quality assurance (EQA) schemes, delivered between 2009 and 2016. Laboratories were provided annually with nine colorectal tumour samples for genotyping. Information on methodology and extent of testing coverage was requested, and scores given for genotyping, interpretation and clerical accuracy. There has been a sixfold increase in laboratory participation (18 in 2009 to 108 in 2016). For RAS genotyping, fewer laboratories now use Roche cobas®, pyrosequencing and Sanger sequencing, with more moving to next generation sequencing (NGS). NGS is the most commonly employed technology for BRAF and PIK3CA mutation screening. KRAS genotyping errors were seen in ≤10% laboratories, until the 2014-2015 scheme, when there was an increase to 16.7%, corresponding to a large increase in scheme participants. NRAS genotyping errors peaked at 25.6% in the first 2015-2016 scheme but subsequently dropped to below 5%. Interpretation and clerical accuracy scores have been consistently good throughout. Within this EQA scheme, we have observed that the quality of molecular analysis for colorectal cancer has continued to improve, despite changes in the required targets, the volume of testing and the technologies employed. It is reassuring to know that laboratories clearly recognise the importance of participating in EQA schemes.
有力证据表明,在为转移性结直肠癌(mCRC)患者开具抗表皮生长因子受体(EGFR)治疗药物之前,应进行扩展的RAS检测。随着越来越多的实验室开展检测,对外部质量保证计划的需求也在增加,从而确保分子分析的高标准。对2009年至2016年间开展的15项英国国家分子遗传学结直肠癌外部质量评估服务(UK NEQAS)外部质量保证(EQA)计划的数据进行了分析。每年为实验室提供9份结直肠肿瘤样本用于基因分型。要求提供有关检测方法和检测覆盖范围的信息,并对基因分型、解读和文书准确性给出评分。实验室参与度增长了六倍(从2009年的18家增至2016年的108家)。对于RAS基因分型,现在使用罗氏cobas®、焦磷酸测序和桑格测序的实验室减少,更多实验室转向了下一代测序(NGS)。NGS是BRAF和PIK3CA突变筛查最常用的技术。在2014 - 2015年计划之前,≤10%的实验室出现KRAS基因分型错误,该计划时这一比例增至16.7%,这与计划参与者大幅增加相对应。NRAS基因分型错误在2015 - 2016年首个计划中达到峰值25.6%,但随后降至5%以下。解读和文书准确性评分一直都很好。在这个EQA计划中,我们观察到,尽管所需检测靶点、检测量和所采用的技术发生了变化,但结直肠癌分子分析的质量仍在持续提高。令人欣慰的是,实验室清楚地认识到参与EQA计划的重要性。