Takano Yoshihiko, Fujino Hisanori, Yachie Akihiro, Sumimoto Shin-Ichi
Department of Pediatrics, Sakai City Medical Center, 1-1-1 Ebaraji-Cho, Nishi-Ku, Sakai City, Osaka, 593-8304, Japan.
Department of Pediatrics, Osaka Red Cross Hospital, 5-30 Fudegasaki-Cho, Tennouji-Ku, Osaka, 543-8555, Japan.
J Med Case Rep. 2017 Jul 2;11(1):178. doi: 10.1186/s13256-017-1317-0.
Sweet's syndrome is characterized by fever, leukocytosis, and tender erythematous papules or nodules. It is a rare condition, particularly in the pediatric population, and has recently been proposed to be an autoinflammatory disease that occurs due to innate immune system dysfunction, involving several cytokines, which causes abnormally increased inflammation. To the best of our knowledge, no report has documented the cytokine profile in a pediatric patient with Sweet's syndrome.
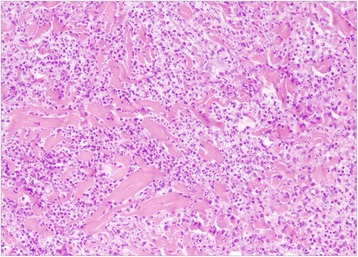
A previously healthy 34-month-old Japanese girl was hospitalized because of remittent fever and pain in her right lower extremity with erythematous nodules. A skin biopsy of the eruption revealed dermal perivascular neutrophilic infiltration with no evidence of vasculitis, which led to the diagnosis of Sweet's syndrome. She was prescribed with orally administered prednisolone and a prompt response was observed; then, the prednisolone dose was tapered. During treatment she developed upper and lower urinary tract infections, after which her cutaneous symptoms failed to improve despite increasing the prednisolone dosage. To avoid long-term use of systemic corticosteroids, orally administered potassium iodide was initiated, but it was unsuccessful. However, orally administered colchicine along with prednisolone effectively ameliorated her symptoms, and prednisolone dosage was reduced again. We analyzed the circulating levels of interleukin-1β, interleukin-6, interleukin-18, neopterin, and soluble tumor necrosis factor receptors I and II, in order to clarify the pathogenesis of Sweet's syndrome. Of these cytokines, only interleukin-6 levels were elevated prior to orally administered prednisolone therapy. Following therapy, the elevated interleukin-6 levels gradually diminished to almost normal levels; interleukin-1β and interleukin-18 stayed within normal ranges throughout the treatment. Neopterin became marginally elevated after the start of treatment. Both soluble tumor necrosis factor receptor I and soluble tumor necrosis factor receptor II levels increased shortly after the onset of urinary tract infections.
This is the first case report of pediatric Sweet's syndrome in which serum cytokine levels were investigated. Future studies should gather more evidence to elucidate the pathophysiology of Sweet's syndrome.
Sweet 综合征的特征为发热、白细胞增多以及压痛性红斑丘疹或结节。它是一种罕见病症,在儿科人群中尤为少见,最近被认为是一种由于先天性免疫系统功能障碍导致的自身炎症性疾病,涉及多种细胞因子,从而引起炎症异常增加。据我们所知,尚无报告记录儿科 Sweet 综合征患者的细胞因子谱。
一名 34 个月大的既往健康日本女孩因弛张热和右下肢疼痛伴红斑结节入院。对皮疹进行皮肤活检显示真皮血管周围中性粒细胞浸润,无血管炎证据,从而诊断为 Sweet 综合征。她接受了口服泼尼松龙治疗,观察到迅速起效;随后,泼尼松龙剂量逐渐减少。治疗期间她发生了上、下尿路感染,此后尽管增加了泼尼松龙剂量,其皮肤症状仍未改善。为避免长期使用全身性皮质类固醇,开始口服碘化钾,但未成功。然而,口服秋水仙碱联合泼尼松龙有效改善了她的症状,泼尼松龙剂量再次减少。我们分析了白细胞介素 -1β、白细胞介素 -6、白细胞介素 -18、蝶呤以及可溶性肿瘤坏死因子受体 I 和 II 的循环水平,以阐明 Sweet 综合征的发病机制。在这些细胞因子中,仅白细胞介素 -6 水平在口服泼尼松龙治疗前升高。治疗后,升高的白细胞介素 -6 水平逐渐降至几乎正常水平;白细胞介素 -1β 和白细胞介素 -18 在整个治疗过程中保持在正常范围内。治疗开始后蝶呤略有升高。可溶性肿瘤坏死因子受体 I 和可溶性肿瘤坏死因子受体 II 水平在尿路感染发作后不久均升高。
这是首例对血清细胞因子水平进行研究的儿科 Sweet 综合征病例报告。未来研究应收集更多证据以阐明 Sweet 综合征的病理生理学。