Schey Steve, Montero Luis Felipe Casado, Stengel-Tosetti Chloe, Gibson Craig J, Dhanasiri Sujith
King's College Hospital, London, UK.
Hospital Virgen de la Salud, Toledo, Spain.
Oncol Ther. 2017;5(1):31-40. doi: 10.1007/s40487-016-0037-8. Epub 2017 Jan 3.
Lenalidomide is an active agent that was approved for use in the EU in 2015 as a first-line therapy for previously untreated, non-transplant eligible multiple myeloma patients. Our objective was to assess the cost impact of lenalidomide when selected as a first-line treatment for transplant-ineligible patients in France, Germany, Italy, Spain, and the United Kingdom (EU5).
We developed a cost-impact model of the total costs associated with newly diagnosed multiple myeloma over 5 years in the EU5 based on treatment duration and time to progression (TTP) (taken from trial data). We compared a baseline scenario (of current lenalidomide uptake) with two alternative future scenarios. Future Scenario A used an increased uptake of first-line lenalidomide: up to 50% in Year 5. Future Scenario B was similar to the baseline, but included a 20% increased uptake of the triple therapy regimen, carfilzomib, lenalidomide, and dexamethasone (KRd) at second line.
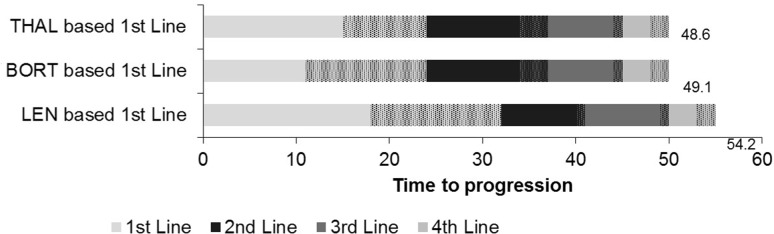
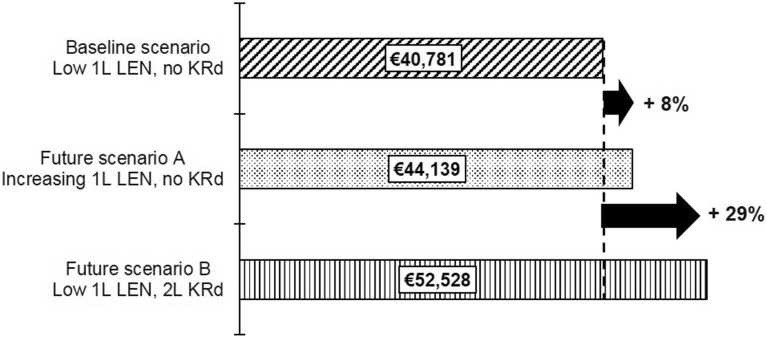
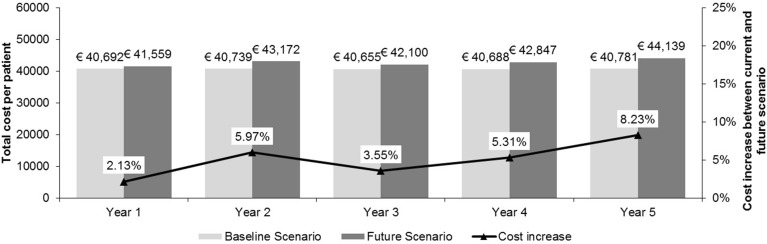
Compared to alternative first-line care pathways, lenalidomide provides a time to progression advantage of up to 5.1 months. In the baseline scenario, the costs per patient were €40,692 in Year 1. Future Scenario A showed an additional expenditure of €867 per patient in Year 1, increasing to €3358 per patient by Year 5, a 2.1% and 8.2% increase from baseline, respectively. However, lenalidomide use was associated with a lower monthly hospitalisation per-patient cost (€813) compared with bortezomib (€1173) and thalidomide (€1532). Future Scenario B was associated with a 29% increase in cost.
Compared to other first line therapies, lenalidomide delays time to progression resulting in associated savings across a patient's treatment pathway and overall is likely to result in a limited impact on budget. Lenalidomide should, therefore, be considered as a first treatment option for multiple myeloma patients ineligible for transplant.
Celgene Ltd.
来那度胺是一种活性药物,于2015年在欧盟获批用于治疗先前未经治疗、不适合移植的多发性骨髓瘤患者的一线治疗。我们的目标是评估来那度胺在法国、德国、意大利、西班牙和英国(欧盟五国)被选为不适合移植患者的一线治疗时的成本影响。
我们基于治疗持续时间和疾病进展时间(TTP)(取自试验数据),建立了一个欧盟五国新诊断多发性骨髓瘤5年总成本的成本影响模型。我们将一个基线情景(当前来那度胺的使用情况)与两个未来替代情景进行了比较。未来情景A使用一线来那度胺的增加使用量:到第5年高达50%。未来情景B与基线相似,但包括二线治疗中三联疗法卡非佐米、来那度胺和地塞米松(KRd)的使用量增加20%。
与替代的一线治疗途径相比,来那度胺可提供长达5.1个月的疾病进展时间优势。在基线情景中,第1年每位患者的成本为40,692欧元。未来情景A显示第1年每位患者额外支出867欧元,到第5年增加到每位患者3358欧元,分别比基线增加2.1%和8.2%。然而,与硼替佐米(1173欧元)和沙利度胺(1532欧元)相比,使用来那度胺每位患者每月的住院成本较低(813欧元)。未来情景B的成本增加了29%。
与其他一线疗法相比,来那度胺延迟了疾病进展时间,从而在患者的整个治疗途径中节省了相关费用,总体上可能对预算产生有限影响。因此,来那度胺应被视为不适合移植的多发性骨髓瘤患者的首选治疗方案。
新基公司