Patorno Elisabetta, Glynn Robert J, Levin Raisa, Lee Moa P, Huybrechts Krista F
Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital, Harvard Medical School, Boston, MA 02120, USA
Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital, Harvard Medical School, Boston, MA 02120, USA.
BMJ. 2017 Jul 6;358:j2941. doi: 10.1136/bmj.j2941.
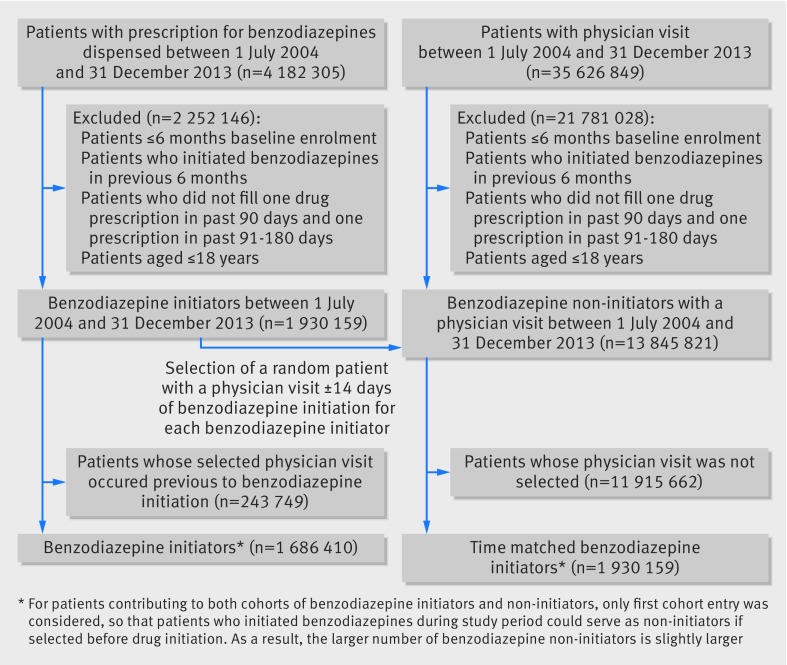
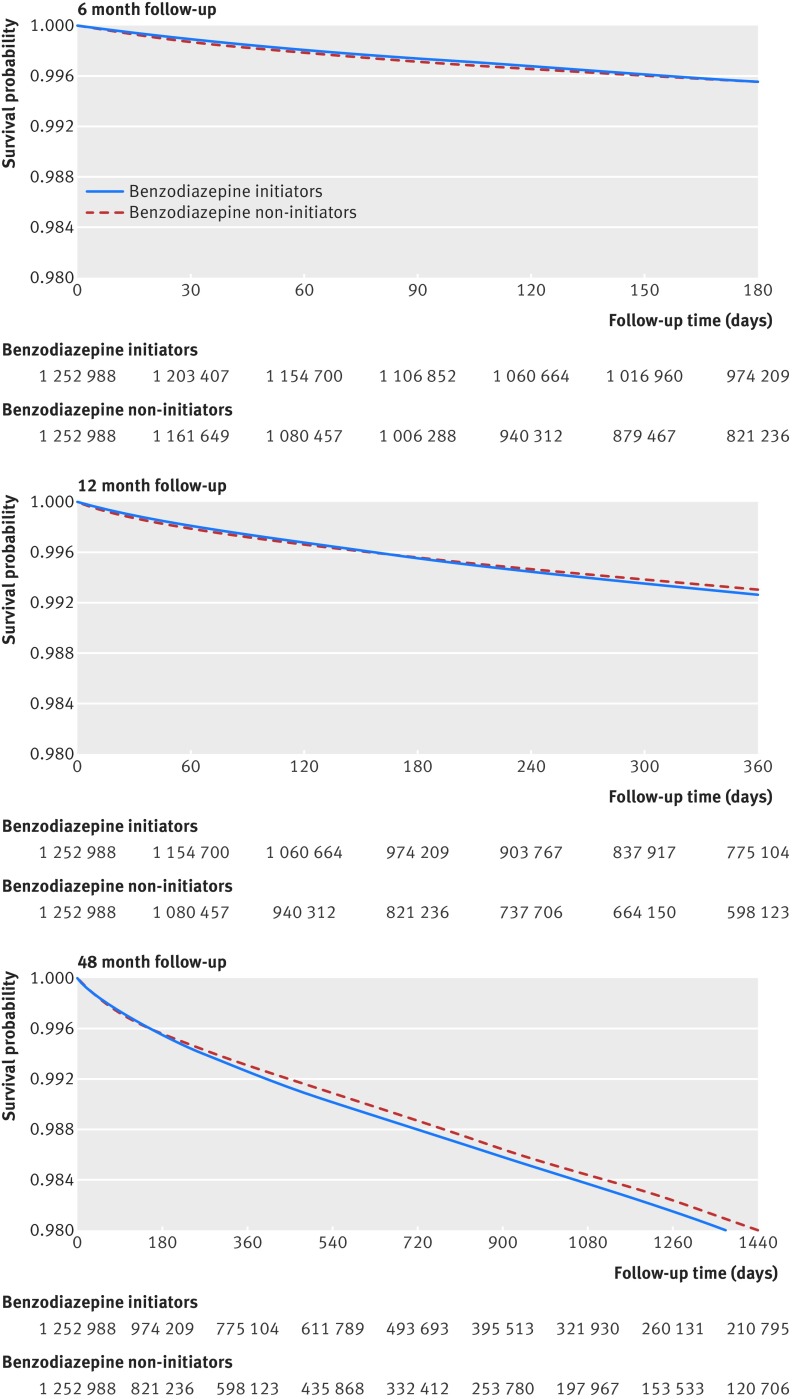
To evaluate the risk of all cause mortality associated with initiating compared with not initiating benzodiazepines in adults, and to address potential treatment barriers and confounding related to the use of a non-active comparator group. Retrospective cohort study. Large de-identified US commercial healthcare database (Optum Clinformatics Datamart). 1:1 high dimensional propensity score matched cohort of benzodiazepine initiators, and randomly selected benzodiazepine non-initiators with a medical visit within 14 days of the start of benzodiazepine treatment (n=1 252 988), between July 2004 and December 2013. To address treatment barriers and confounding, patients were required to have filled one or more prescriptions for any medication in the 90 days and 91-180 days before the index date (ie, the date of starting benzodiazepine treatment for initiators and the date of the selected medical visit for benzodiazepine non-initiators) and the high dimensional propensity score was estimated on the basis of more than 300 covariates. All cause mortality, determined by linkage with the Social Security Administration Death Master File. Over a six month follow-up period, 5061 and 4691 deaths occurred among high dimensional propensity score matched benzodiazepine initiators versus non-initiators (9.3 9.4 events per 1000 person years; hazard ratio 1.00, 95% confidence interval 0.96 to 1.04). A 4% (95% confidence interval 1% to 8%) to 9% (2% to 7%) increase in mortality risk was observed associated with the start of benzodiazepine treatment for follow-ups of 12 and 48 months and in subgroups of younger patients and patients initiating short acting agents. In secondary analyses comparing 1:1 high dimensional propensity score matched patients initiating benzodiazepines with an active comparator, ie, patients starting treatment with selective serotonin reuptake inhibitor antidepressants, benzodiazepine use was associated with a 9% (95% confidence interval 3% to 16%) increased risk. This large population based cohort study suggests either no increase or at most a minor increase in risk of all cause mortality associated with benzodiazepine initiation. If a detrimental effect exists, it is likely to be much smaller than previously stated and to have uncertain clinical relevance. Residual confounding likely explains at least part of the small increase in mortality risk observed in selected analyses.
为评估在成年人中开始使用苯二氮䓬类药物与未开始使用相比的全因死亡风险,并解决与使用非活性对照人群相关的潜在治疗障碍和混杂因素。回顾性队列研究。使用美国一个大型匿名商业医疗保健数据库(Optum Clinformatics Datamart)。在2004年7月至2013年12月期间,对苯二氮䓬类药物起始者进行1:1高维倾向评分匹配队列研究,并随机选择在苯二氮䓬类药物治疗开始后14天内有就诊记录的未使用苯二氮䓬类药物者(n = 1252988)。为解决治疗障碍和混杂因素,要求患者在索引日期(即起始者开始使用苯二氮䓬类药物的日期和未使用苯二氮䓬类药物者选定就诊日期)前90天和91 - 180天内已开具一种或多种任何药物的处方,并根据300多个协变量估计高维倾向评分。通过与社会保障管理局死亡主文件进行关联确定全因死亡率。在六个月的随访期内,高维倾向评分匹配的苯二氮䓬类药物起始者和未使用者中分别有5061例和4691例死亡(每1000人年9.3和9.4例事件;风险比1.00,95%置信区间0.96至1.04)。在12个月和48个月的随访以及年轻患者和开始使用短效药物的患者亚组中,观察到与开始使用苯二氮䓬类药物治疗相关的死亡风险增加4%(95%置信区间1%至8%)至9%(2%至7%)。在将开始使用苯二氮䓬类药物的1:1高维倾向评分匹配患者与活性对照(即开始使用选择性5-羟色胺再摄取抑制剂抗抑郁药治疗的患者)进行比较的二次分析中,使用苯二氮䓬类药物与风险增加9%(95%置信区间3%至16%)相关。这项基于大量人群的队列研究表明,与开始使用苯二氮䓬类药物相关的全因死亡风险要么没有增加,要么至多有轻微增加。如果存在有害影响,其可能比先前所述的要小得多,且临床相关性不确定。残留混杂因素可能至少部分解释了在选定分析中观察到的死亡风险的小幅增加。