Win Sithu, Hussain Imad, Hebl Virginia B, Dunlay Shannon M, Redfield Margaret M
From the Department of Cardiovascular Disease, Division of Circulatory Failure, Mayo Clinic, Rochester, MN. Current address for Dr Hussain: Department of Medicine, Division of Cardiology, Houston Methodist Hospital, Houston, TX. Current address for Dr Hebl: Department of Medicine, Division of Cardiovascular Disease, Oregon Health & Science University, Portland, OR.
Circ Heart Fail. 2017 Jul;10(7). doi: 10.1161/CIRCHEARTFAILURE.117.003926.
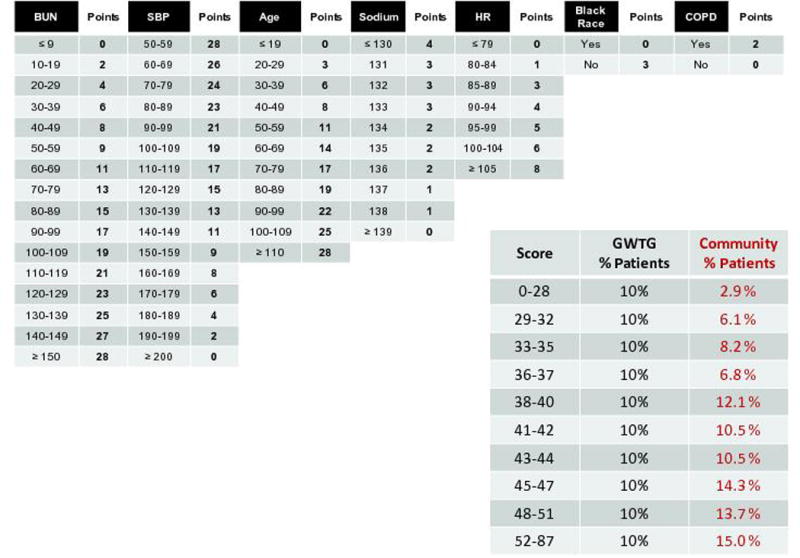
The Acute Decompensated Heart Failure National Registry (ADHERE) and Get With The Guidelines (GWTG) registries have developed simple heart failure (HF) in-hospital mortality risk scores. We hypothesized that HF scores predictive of in-hospital mortality would perform as well for early postdischarge mortality risk stratification.
In this single-center, community-based, retrospective study of all consecutive primary HF hospitalizations (6203 hospitalizations in 3745 patients) from 2000 to 2013, the ADHERE and GWTG risk scores were calculated from admission data. There were 176 (3.0%) and 399 (6.7%), 869 (14.7%), and 1272 (21.5%) deaths in-hospital and at 30, 90, and 180 days postdischarge, respectively. The GWTG but not ADHERE risk score was well calibrated for in-hospital mortality. Both the ADHERE (C statistic 0.66 and 0.67, 0.64, and 0.64) and GWTG (C statistic 0.74 and 0.73, 0.71, and 0.70) HF risk scores were similarly predictive of in-hospital and 30-, 90-, and 180-day postdischarge mortality. The ADHERE risk score identified 10% and the GWTG risk score identified 20% of hospitalizations where 180-day postdischarge mortality was 50%, a prognostic bench mark for hospice referral. In contrast, hospitalizations characterized as lowest risk by the ADHERE (57% of hospitalizations; 180-day mortality 16.2%) or GWTG score (20% of hospitalizations; 180-day mortality 8.0%) had substantially lower mortality (odds ratios high versus low risk of 5-8 [ADHERE] and 11-18 [GWTG] across time points; <0.0001 for all).
The simple ADHERE and GWTG scores stratify hospitalized HF patients for both inpatient and early postdischarge mortality risk, allowing comprehensive risk assessment on admission.
急性失代偿性心力衰竭国家注册登记处(ADHERE)和遵循指南(GWTG)注册登记处已制定了简单的心力衰竭(HF)院内死亡风险评分。我们假设,预测院内死亡的HF评分对于出院后早期死亡风险分层同样有效。
在这项基于社区的单中心回顾性研究中,纳入了2000年至2013年期间所有连续性原发性HF住院患者(3745例患者中的6203次住院),根据入院数据计算ADHERE和GWTG风险评分。分别有176例(3.0%)、399例(6.7%)、869例(14.7%)和1272例(21.5%)患者在住院期间、出院后30天、90天和180天死亡。GWTG风险评分(而非ADHERE风险评分)对于院内死亡具有良好的校准度。ADHERE(C统计量分别为0.66、0.67、0.64和0.64)和GWTG(C统计量分别为0.74、0.73、0.71和0.70)HF风险评分对于院内以及出院后30天、90天和180天死亡同样具有预测性。ADHERE风险评分识别出10%的住院患者,GWTG风险评分识别出20%的住院患者,这些患者出院后180天死亡率为50%,这是临终关怀转诊的一个预后基准。相比之下,ADHERE(占住院患者的57%;180天死亡率16.2%)或GWTG评分(占住院患者的20%;180天死亡率8.0%)所确定的低风险住院患者死亡率显著更低(不同时间点高风险与低风险的比值比,ADHERE为5至8,GWTG为11至18;所有均<0.0001)。
简单的ADHERE和GWTG评分可对住院HF患者的住院期间及出院后早期死亡风险进行分层,从而在入院时进行全面的风险评估。