Department of Cardiology, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, China.
School of Medicine, Southeast University, Nanjing, China.
ESC Heart Fail. 2023 Feb;10(1):502-517. doi: 10.1002/ehf2.14208. Epub 2022 Nov 3.
The aim of this study was to assess the performance of these main scores in predicting prognosis in patients with heart failure (HF).
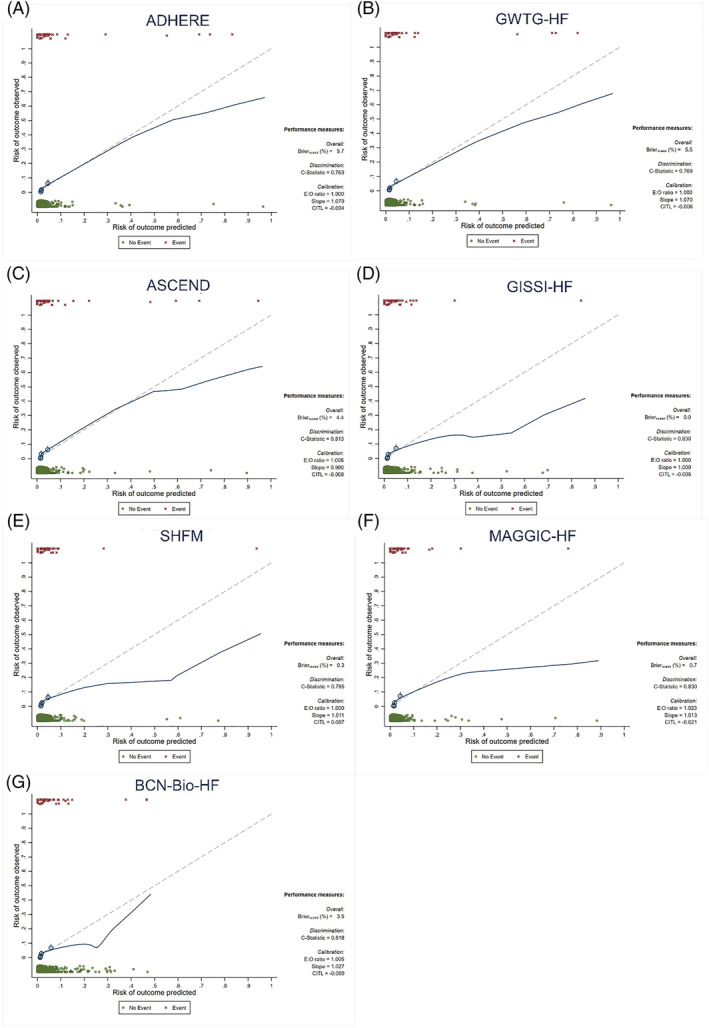
A total of 2008 patients who were admitted to the Fourth People's Hospital of Zigong, Sichuan, from December 2016 to June 2019 and diagnosed with HF were included in the study. We compared the prognostic predictive performance of Seattle Heart Failure Model (SHFM), Meta-Analysis Global Group in Chronic Heart Failure (MAGGIC-HF) risk score, Get With the Guidelines-Heart Failure programme (GWTG-HF), Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure (ASCEND) risk scores, the Acute Decompensated Heart Failure National Registry (ADHERE) model, Barcelona Bio-Heart Failure (BCN-Bio-HF) risk calculator, and Gruppo Italiano per lo Studio della Streptochinasi nell'Infarto Miocardico-Heart Failure (GISSI-HF) for the endpoints. The primary endpoint was 1 year all-cause mortality and the secondary endpoint was the incidence of 28 day readmission post-discharge. At 1 year follow-up, 44 (2.21%) patients with HF died. Discrimination analyses showed that all risk scores performed reasonably well in predicting 1 year mortality, with areas under the receiver operating characteristic curve (AUCs) fluctuating between 0.757 and 0.822. GISSI-HF showed the best discrimination with the AUC of 0.822 (0.768-0.876), followed by MAGGIC-HF, BCN-Bio-HF, ASCEND, SHFM, GWTG-HF, and ADHERE with AUCs of 0.819 (0.756-0.883), 0.812 (0.758-0.865), 0.802 (0.742-0.862), 0.787 (0.725-0.849), 0.762 (0.684-0.840), and 0.757 (0.681-0.833), respectively. All risk scores were similarly predictive of 28 day emergency readmissions, with AUCs fluctuating between 0.609 and 0.680. Overestimation of mortality occurred in all scores except the ASCEND. The risk scores remained with good prognostic discrimination in patients with biventricular HF and in the subgroup of patients taking angiotensin-converting enzyme inhibitor/angiotensin II receptor blocker.
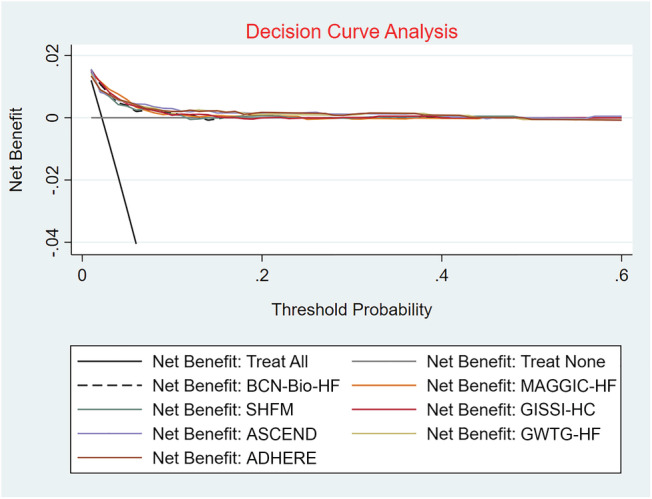
Currently assessed risk scores have limited clinical utility, with fair accuracy and calibration in assessing patients' 1 year risk of death and poor accuracy in assessing patients' risk of readmission. There is a need to incorporate more patient-level information, use more advanced technologies, and develop models for different subgroups of patients to achieve more practical, innovative, and accurate risk assessment tools.
本研究旨在评估这些主要评分系统在预测心力衰竭(HF)患者预后方面的表现。
共纳入 2008 例 2016 年 12 月至 2019 年 6 月在四川自贡市第四人民医院就诊并诊断为 HF 的患者。我们比较了西雅图心力衰竭模型(SHFM)、Meta 分析全球慢性心力衰竭专家组(MAGGIC-HF)风险评分、遵循指南-心力衰竭项目(GWTG-HF)、急性失代偿性心力衰竭中奈西立肽临床疗效的临床研究(ASCEND)风险评分、急性失代偿性心力衰竭国家登记(ADHERE)模型、巴塞罗那生物心力衰竭风险计算器(BCN-Bio-HF)和意大利心肌梗死后应用链激酶治疗的研究组-心力衰竭(GISSI-HF)在终点方面的预后预测性能。主要终点为 1 年全因死亡率,次要终点为出院后 28 天再入院发生率。在 1 年随访时,44 例(2.21%)HF 患者死亡。判别分析显示,所有风险评分在预测 1 年死亡率方面均表现良好,受试者工作特征曲线下面积(AUCs)在 0.757 至 0.822 之间波动。GISSI-HF 具有最佳的判别能力,AUC 为 0.822(0.768-0.876),其次是 MAGGIC-HF、BCN-Bio-HF、ASCEND、SHFM、GWTG-HF 和 ADHERE,AUC 分别为 0.819(0.756-0.883)、0.812(0.758-0.865)、0.802(0.742-0.862)、0.787(0.725-0.849)、0.762(0.684-0.840)和 0.757(0.681-0.833)。所有风险评分对 28 天急诊再入院的预测能力相似,AUC 在 0.609 至 0.680 之间波动。除 ASCEND 外,所有评分均存在死亡率高估。在双心室 HF 患者和使用血管紧张素转换酶抑制剂/血管紧张素 II 受体阻滞剂的患者亚组中,风险评分仍具有良好的预后判别能力。
目前评估的风险评分在评估患者 1 年死亡风险方面具有有限的临床应用价值,其准确性和校准度均为中等,而在评估患者再入院风险方面准确性较差。需要纳入更多患者层面的信息,使用更先进的技术,并为不同患者亚组开发模型,以实现更实用、创新和准确的风险评估工具。