Shaddock Erica J
Division of Pulmonology and Critical Care, Department of Internal Medicine, Area 552 Charlotte Maxeke Johannesburg Academic Hospital, Jubilee Road, Parktown, Johannesburg, 2193 South Africa.
Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Pneumonia (Nathan). 2016 Oct 28;8:17. doi: 10.1186/s41479-016-0017-7. eCollection 2016.
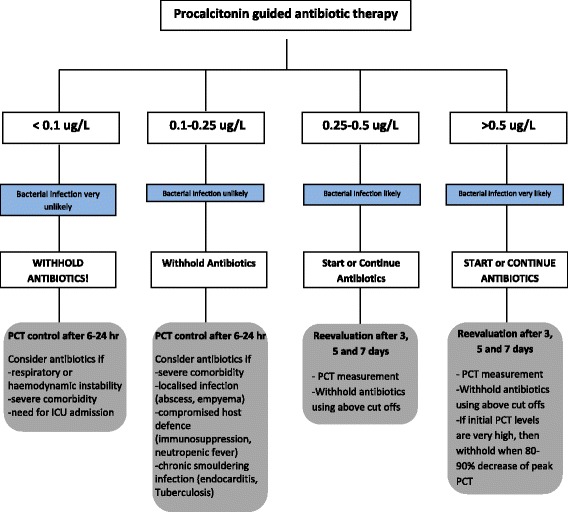
Community-acquired pneumonia (CAP) is a leading cause of death in both the developed and developing world. The very young and elderly are especially vulnerable. Even with appropriate early antibiotics we still have not improved the outcomes in these patients since the 1950s, with 30-day case fatality rates of between 10-12%. Interventions to improve outcomes include immunomodulatory agents such as macrolides and corticosteroids. Treating doctors identify CAP patients who are likely to have poor outcomes by using severity scores such as the pneumonia severity index and CURB-65, which allows these patients to be placed in ICU settings from the start of the admission. Another novel way to identify these patients is with the use of biomarkers. This review illustrates how various biomarkers have been shown to predict mortality, complications and response to treatment in CAP patients. The evidence using either procalcitonin or C-reactive protein to demonstrate response to treatment and hence that the antibiotics chosen are appropriate can play an important role in antibiotic stewardship.
社区获得性肺炎(CAP)是发达国家和发展中国家的主要死因。婴幼儿和老年人尤其易受影响。自20世纪50年代以来,即使使用了适当的早期抗生素,我们仍未改善这些患者的治疗结果,30天病死率在10%至12%之间。改善治疗结果的干预措施包括免疫调节剂,如大环内酯类药物和皮质类固醇。治疗医生通过使用诸如肺炎严重程度指数和CURB-65等严重程度评分来识别可能预后不良的CAP患者,这使得这些患者从入院开始就可以被安置在重症监护病房。另一种识别这些患者的新方法是使用生物标志物。这篇综述阐述了各种生物标志物如何被证明可预测CAP患者的死亡率、并发症及对治疗的反应。使用降钙素原或C反应蛋白来证明对治疗的反应,从而表明所选抗生素合适,这一证据在抗生素管理中可发挥重要作用。