Calder Lisa Anne, Mastoras George, Rahimpour Mitra, Sohmer Benjamin, Weitzman Brian, Cwinn A Adam, Hobin Tara, Parush Avi
Department of Emergency Medicine, The Ottawa Hospital, Civic Campus, 1053 Carling Avenue, E-Main, Room EM-206, Box 227, Ottawa, Ontario, K1Y 4E9, Canada.
Clinical Epidemiology Program, Ottawa Hospital Research Institute, 1053 Carling Avenue, Room F6-58, Ottawa, Ontario, K1Y 4E9, Canada.
Int J Emerg Med. 2017 Dec;10(1):24. doi: 10.1186/s12245-017-0149-4. Epub 2017 Jul 14.
In order to enhance patient safety during resuscitation of critically ill patients, we need to optimize team communication and enhance team situational awareness but little is known about resuscitation team communication patterns. The objective of this study is to understand how teams communicate during resuscitation; specifically to assess for a shared mental model (organized understanding of a team's relationships) and information needs.
We triangulated 3 methods to evaluate resuscitation team communication at a tertiary care academic trauma center: (1) interviews; (2) simulated resuscitation observations; (3) live resuscitation observations. We interviewed 18 resuscitation team members about shared mental models, roles and goals of team members and procedural expectations. We observed 30 simulated resuscitation video recordings and documented the timing, source and destination of communication and the information category. We observed 12 live resuscitations in the emergency department and recorded baseline characteristics of the type of resuscitations, nature of teams present and type and content of information exchanges. The data were analyzed using a qualitative communication analysis method.
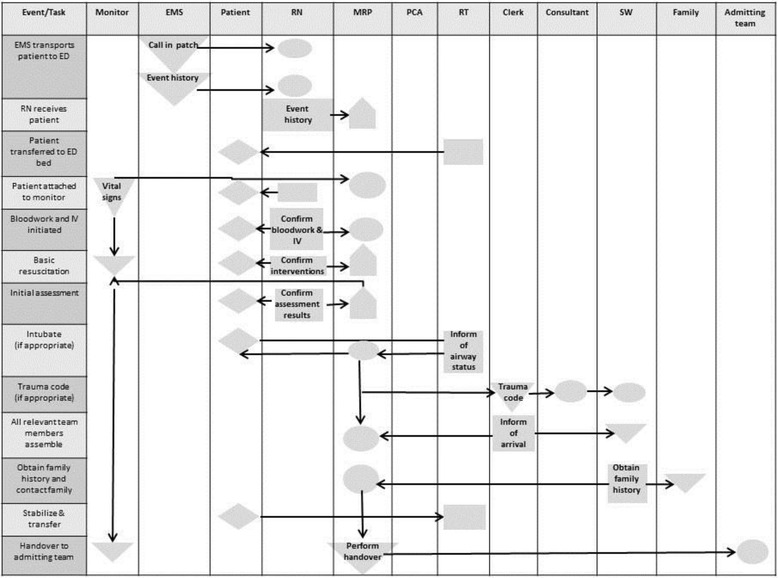
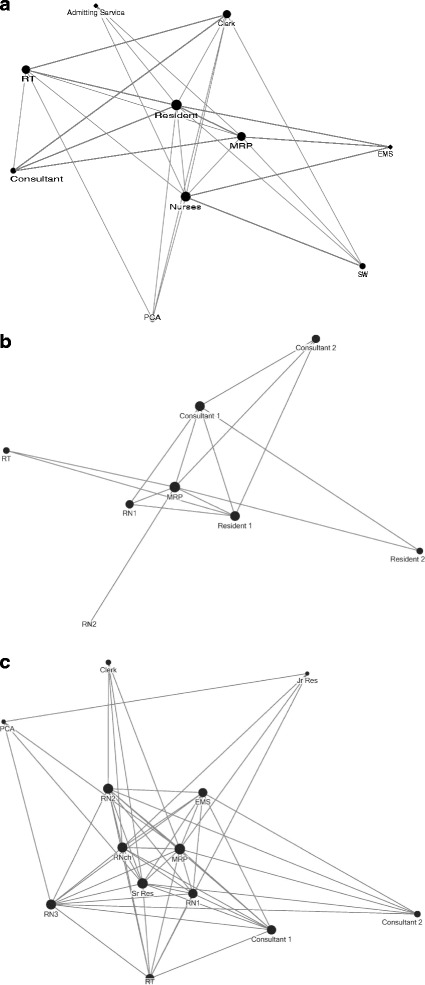
We found that resuscitation team members described a shared mental model. Respondents understood the roles and goals of each team member in order to provide rapid, efficient and life-saving care with an overall need for situational awareness. The information flow described in the interviews was reflected during the simulated and live resuscitations with the most responsible physician and charting nurse being central to team communication. We consolidated communicated information into six categories: (1) time; (2) patient status; (3) patient history; (4) interventions; (5) assistance and consultations; 6) team members present.
Resuscitation team members expressed a shared mental model and prioritized situational awareness. Our findings support a need for cognitive aids to enhance team communication during resuscitations.
为了在危重症患者复苏过程中提高患者安全性,我们需要优化团队沟通并增强团队态势感知能力,但对于复苏团队的沟通模式却知之甚少。本研究的目的是了解团队在复苏过程中如何进行沟通;具体而言,是评估共享心智模型(对团队关系的有组织理解)和信息需求。
我们采用三种方法对一家三级医疗学术创伤中心的复苏团队沟通进行三角测量:(1)访谈;(2)模拟复苏观察;(3)现场复苏观察。我们就共享心智模型、团队成员的角色和目标以及程序期望对18名复苏团队成员进行了访谈。我们观察了30段模拟复苏视频记录,并记录了沟通的时间、来源和目的地以及信息类别。我们在急诊科观察了12次现场复苏,并记录了复苏类型的基线特征、在场团队的性质以及信息交流的类型和内容。数据采用定性沟通分析方法进行分析。
我们发现复苏团队成员描述了一种共享心智模型。受访者理解每个团队成员的角色和目标,以便提供快速、高效和挽救生命的护理,并总体上需要态势感知。访谈中描述的信息流在模拟和现场复苏过程中得到了体现,最负责的医生和记录护士是团队沟通的核心。我们将沟通的信息归纳为六类:(1)时间;(2)患者状态;(3)患者病史;(4)干预措施;(5)协助与会诊;(6)在场团队成员。
复苏团队成员表达了一种共享心智模型,并将态势感知作为优先事项。我们的研究结果支持在复苏过程中需要认知辅助工具来增强团队沟通。