Takagishi Seesha R, Marx Tessa E, Lewis Christopher, Tarabadkar Erica S, Juhlin Ilsa D, Blom Astrid, Iyer Jayasri G, Liao Jay J, Tseng Yolanda D, Fu Teresa, Nghiem Paul, Parvathaneni Upendra
Department of Medicine/Dermatology, University of Washington, Seattle, Washington.
Department of Radiation Oncology, University of Washington, Seattle, Washington.
Adv Radiat Oncol. 2016 Oct 20;1(4):244-251. doi: 10.1016/j.adro.2016.10.003. eCollection 2016 Oct-Dec.
Merkel cell carcinoma (MCC) is a rare and often aggressive skin cancer. Typically, surgery is the primary treatment. Postoperative radiation therapy (PORT) is often recommended to improve local control. It is unclear whether PORT is indicated in patients with favorable Stage IA head and neck (HN) MCC.
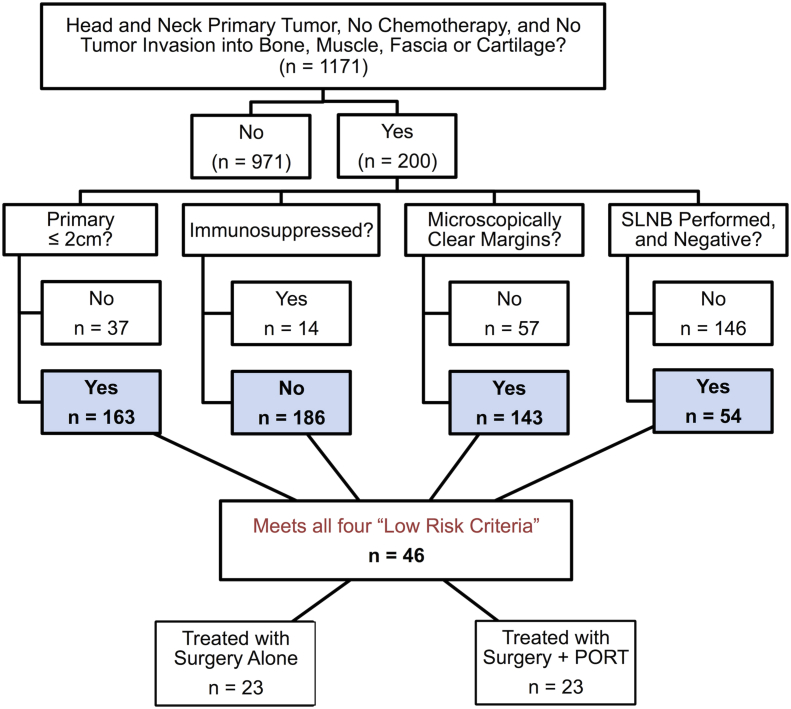
We conducted a retrospective analysis of 46 low-risk HN MCC cases treated between 2006 and 2015. Inclusion criteria were defined as a primary tumor size of ≤ 2 cm, negative pathological margins, negative sentinel lymph node biopsy, and no immunosuppression. Local recurrence (LR) was defined as tumor recurrence within 2 cm of the primary surgical bed and estimated with the Kaplan-Meier method.
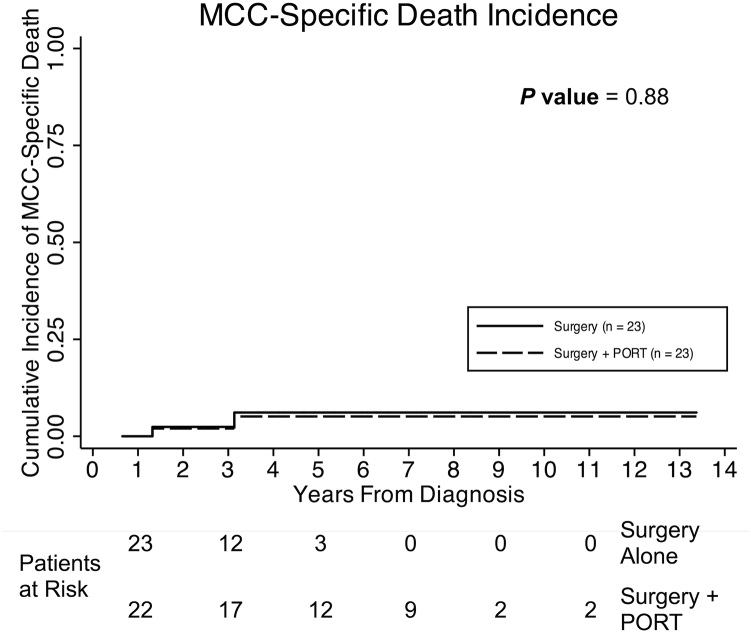
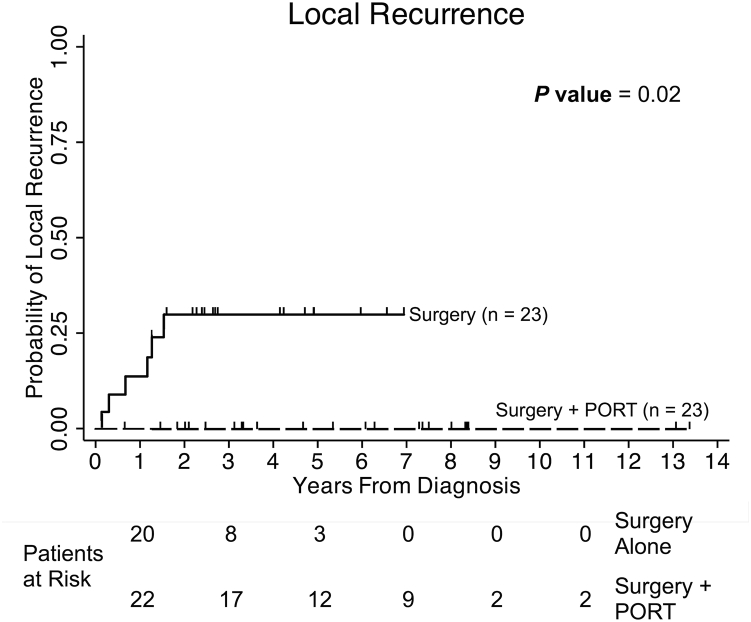
Omission of PORT was offered to all 46 patients, of which 23 patients received PORT and 23 did not. No patient received adjuvant chemotherapy. There were no significant differences in surgical margins, tumor size, depth, lympho-vascular invasion status, or demographics between the two patient groups. Median follow-up for all patients was 3.7 years. Six of the 23 patients who did not receive PORT developed an LR. Compared to the group that received PORT, there was a significantly higher risk of LR in the group treated without PORT (26% vs. 0%, = .02). Median time to LR was 11 months. All local failures were effectively salvaged. There was no difference in MCC-specific and overall survival between the 2 groups.
For patients with HN MCC, omission of PORT was associated with a significantly higher risk of local recurrence even among those patients with the lowest-risk tumors (i.e., Stage IA without immune suppression). Thus, it is important to weigh the benefits of PORT against the side effect profile on a case-specific basis for each patient.
默克尔细胞癌(MCC)是一种罕见且通常具有侵袭性的皮肤癌。通常,手术是主要治疗方法。术后放射治疗(PORT)常被推荐用于改善局部控制。目前尚不清楚PORT是否适用于IA期头颈部(HN)MCC的低风险患者。
我们对2006年至2015年间治疗的46例低风险HN MCC病例进行了回顾性分析。纳入标准定义为原发肿瘤大小≤2 cm、病理切缘阴性、前哨淋巴结活检阴性且无免疫抑制。局部复发(LR)定义为原发手术床2 cm内的肿瘤复发,并采用Kaplan-Meier方法进行估计。
46例患者均被建议不进行PORT,其中23例患者接受了PORT,23例未接受。所有患者均未接受辅助化疗。两组患者在手术切缘、肿瘤大小、深度、淋巴管浸润状态或人口统计学特征方面无显著差异。所有患者的中位随访时间为3.七年。23例未接受PORT的患者中有6例发生了LR。与接受PORT的组相比,未接受PORT治疗的组发生LR的风险显著更高(26%对0%,P =.02)。LR的中位时间为11个月。所有局部复发均得到有效挽救。两组之间的MCC特异性生存率和总生存率无差异。
对于HN MCC患者,即使在肿瘤风险最低的患者(即无免疫抑制的IA期)中,不进行PORT也与显著更高的局部复发风险相关。因此,根据每个患者的具体情况权衡PORT的益处与副作用是很重要的。