McNew Laura K, Bowen Stephen R, Gopan Olga, Nyflot Matthew J, Patel Shilpen A, Zeng Jing, Rengan Ramesh
Department of Radiation Oncology, University of Washington Medical Center, Seattle, Washington.
Adv Radiat Oncol. 2017 Feb 1;2(2):192-196. doi: 10.1016/j.adro.2017.01.008. eCollection 2017 Apr-Jun.
The results from Radiation Therapy Oncology Group (RTOG) 0617, a dose escalation trial that compared treatment with 60 Gy versus 74 Gy for patients with stage III non-small cell lung cancer (NSCLC), suggested that in these patients, the heart dose from radiation therapy correlates with survival. In particular, the study noted that patients with a high heart V5 and V30 had a poorer overall survival; however, the exact cause of this correlation is not known. We hypothesize that heart dose may be a surrogate for mediastinal nodal involvement, which has prognostic value in NSCLC. This study evaluates the relationship between heart dose and involvement of mediastinal lymph nodes in patients with stage III NSCLC treated with radiation therapy.
A total of 56 patients were identified and treated with definitive radiation therapy from 2007 to 2014. The heart was recontoured for every patient by a single physician, per the RTOG 1106 contouring atlas. We assessed lymph node station involvement using pretreatment data, and nodal coverage was confirmed on plan review.
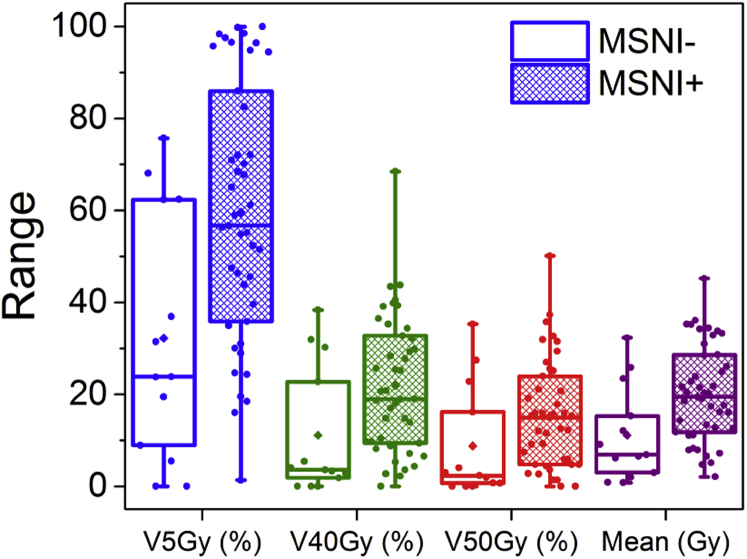
Mean heart dose was found to be significantly higher in patients with multinodal station and level 7 involvement. On Spearman's rank correlation, level 7 was significantly associated with all heart parameters tested ( < .001). Patients who had 2 or more lymph node stations involved were found to have significantly higher heart doses for all parameters tested when compared with those who had only one station involved or no nodal involvement.
Our findings suggest that heart dose may be a surrogate for other prognostic factors in stage III NSCLC rather than an independent predictor of outcome.
放射治疗肿瘤学组(RTOG)0617试验是一项剂量递增试验,比较了III期非小细胞肺癌(NSCLC)患者接受60 Gy与74 Gy治疗的效果,结果表明,在这些患者中,放射治疗对心脏的剂量与生存率相关。特别是,该研究指出,心脏V5和V30较高的患者总生存率较差;然而,这种相关性的确切原因尚不清楚。我们假设心脏剂量可能是纵隔淋巴结受累的替代指标,而纵隔淋巴结受累在NSCLC中具有预后价值。本研究评估了接受放射治疗的III期NSCLC患者心脏剂量与纵隔淋巴结受累之间的关系。
共纳入56例患者,于2007年至2014年接受了根治性放射治疗。由一名医生根据RTOG 1106轮廓图集为每位患者重新勾勒心脏轮廓。我们使用治疗前数据评估淋巴结站受累情况,并在计划审查时确认淋巴结覆盖情况。
发现多站和7级受累患者的平均心脏剂量显著更高。在Spearman等级相关性分析中,7级与所有测试的心脏参数均显著相关(P <.001)。与仅累及一个淋巴结站或无淋巴结受累的患者相比,发现累及2个或更多淋巴结站的患者在所有测试参数中的心脏剂量均显著更高。
我们的研究结果表明,心脏剂量可能是III期NSCLC其他预后因素的替代指标,而不是结果的独立预测因素。