Macomber Meghan W, Bowen Stephen R, Gopan Olga, Yeung Rosanna, Apisarnthanarax Smith, Zeng Jing, Patel Shilpen
Radiation Oncology, University of Washington Medical Center, Seattle, USA.
Radiation Oncology, University of Washington/Seattle Cancer Care Alliance Proton Therapy Center, Seattle, USA.
Cureus. 2018 Mar 27;10(3):e2378. doi: 10.7759/cureus.2378.
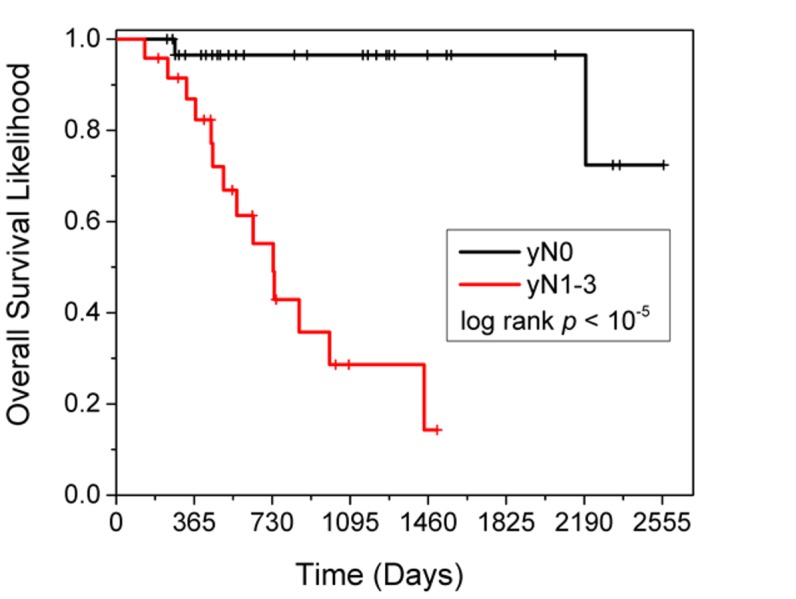
Purpose Studies have shown that radiation dose to the heart may be associated with worse outcomes in patients receiving chemoradiation for lung cancer. As esophageal cancer radiation treatment can result in relatively high cardiac doses, we evaluated a single-institution database of patients treated for esophageal cancer for heart dose and outcomes. Methods We retrospectively reviewed 59 patients with stage IIA-IIIB esophageal cancer treated with neoadjuvant chemoradiation to 50.4 Gy followed by esophagectomy from 2007-2015. Patient demographics and outcome data, including pathological response, local recurrence, distant metastases, and overall survival, were obtained. Mean heart dose (MHD), heart V5, V40, and V50, were calculated. Differences in patient characteristics between the three radiation therapy modalities: three-dimensional (3D) conformal radiotherapy (3D-CRT), intensity modulated radiotherapy (IMRT), and proton beam radiation therapy (PBT) were tested using non-parametric Kruskal-Wallis (K-W) analysis of variance (ANOVA). Patient characteristics and heart dosimetric parameters were screened by univariate Cox regression for an association to overall survival, and univariate predictors (p < 0.05) were then selected as inputs into a multivariate Cox regression model using stepwise backward elimination. Kaplan-Meier risk-stratified survival curves were plotted for the best univariate or multivariate Cox model variables. An exploratory subgroup univariate Cox regression was conducted in each of the treatment modalities (proton, IMRT, 3D-CRT). Results The median follow-up was 20 months. The median overall survival was 73 months. Eleven patients (20%) experienced a complete pathologic response (pCR). Only two patients (4%) experienced a local recurrence. On univariate analysis, predictors of survival were age, prior radiation, pathologic response in involved lymph nodes, and tumor length post-treatment. On a multivariate analysis, only pathologic nodal response (yN) remained significant (p = 0.007). There was no relationship between any heart dosimetric variables analyzed and any clinical outcomes. Conclusions In this retrospective review, radiation dose to the heart was not associated with inferior treatment outcomes in patients receiving trimodality therapy for esophageal cancer.
目的 研究表明,肺癌接受放化疗患者的心脏辐射剂量可能与较差的预后相关。由于食管癌放射治疗可导致相对较高的心脏剂量,我们评估了一个单机构食管癌治疗患者数据库中的心脏剂量和预后情况。方法 我们回顾性分析了2007年至2015年间59例IIA-IIIB期食管癌患者,这些患者接受了新辅助放化疗,剂量为50.4 Gy,随后进行了食管切除术。获取了患者的人口统计学和预后数据,包括病理反应、局部复发、远处转移和总生存期。计算了平均心脏剂量(MHD)、心脏V5、V40和V50。使用非参数Kruskal-Wallis(K-W)方差分析(ANOVA)检验了三种放射治疗方式(三维(3D)适形放疗(3D-CRT)、调强放疗(IMRT)和质子束放疗(PBT))之间患者特征的差异。通过单变量Cox回归筛选患者特征和心脏剂量学参数与总生存期的关联,然后将单变量预测因子(p < 0.05)作为输入,使用逐步向后排除法纳入多变量Cox回归模型。为最佳单变量或多变量Cox模型变量绘制Kaplan-Meier风险分层生存曲线。在每种治疗方式(质子、IMRT、3D-CRT)中进行探索性子组单变量Cox回归。结果 中位随访时间为20个月。中位总生存期为73个月。11例患者(20%)出现完全病理缓解(pCR)。仅2例患者(4%)出现局部复发。单变量分析中,生存的预测因子为年龄、既往放疗、受累淋巴结的病理反应和治疗后肿瘤长度。多变量分析中,仅病理淋巴结反应(yN)仍具有显著性(p = 0.007)。所分析的任何心脏剂量学变量与任何临床结局之间均无关联。结论 在这项回顾性研究中,食管癌接受三联疗法患者的心脏辐射剂量与较差的治疗结局无关。