Urology Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Department of Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH, USA.
Eur Urol Focus. 2018 Jan;4(1):100-105. doi: 10.1016/j.euf.2016.07.006. Epub 2016 Jul 28.
Clear cell renal cell carcinoma (RCC) continues to be the most commonly diagnosed subtype and is associated with more aggressive behavior than papillary and chromophobe RCC. Predicting disease recurrence after surgical extirpation is important for counseling and targeting those at high risk for adjuvant therapy clinical trials.
To validate a postoperative nomogram predicting 5-yr recurrence-free probability (RFP) for clinically localized clear cell RCC.
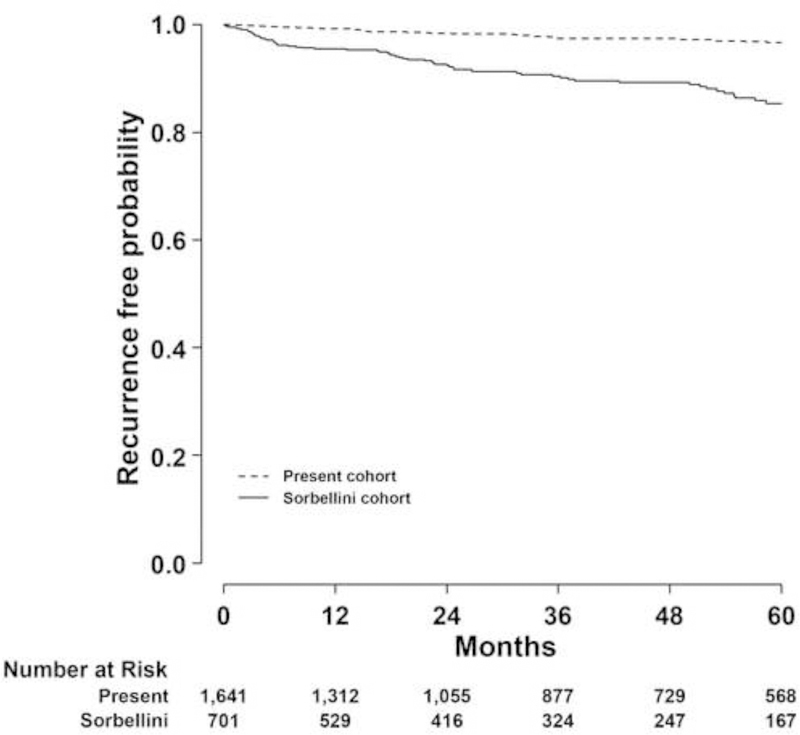
DESIGN, SETTING, AND PARTICIPANTS: We identified all patients who underwent nephrectomy for clinically localized clear cell RCC from 1990 to 2009 at Memorial Sloan Kettering Cancer Center. After excluding patients with bilateral renal masses, familial RCC syndromes, and T3c or T4 tumors due to the limited number, 1642 participants were available for analysis.
Partial or radical nephrectomy.
Disease recurrence was defined as any new tumor after nephrectomy or kidney cancer-specific mortality, whichever occurred first. A postoperative nomogram was used to calculate the predicted 5-yr RFP, and these values were compared with the actual 5-yr RFP. Nomogram performance was evaluated by concordance index and calibration plot.
Median follow-up was 39 mo (interquartile range: 14-79 mo), and disease recurrence was observed in 50 patients. The nomogram concordance index was 0.81. The calibration curve showed that the nomogram underestimated the actual 5-yr RFP. We updated the nomogram by including the entire patient population, which maintained performance and significantly improved calibration.
The updated clear cell RCC postoperative nomogram performed well in the combined cohort. Underestimation of actual 5-yr RFP by the original nomogram may be due to increased surgeon experience and other unknown variables.
We updated a valuable prediction tool used for assessing the disease recurrence probability after nephrectomy for clear cell renal cell carcinoma.
透明细胞肾细胞癌(RCC)仍然是最常见的诊断亚型,其行为比乳头状和嫌色性 RCC 更具侵袭性。预测手术后疾病复发对于咨询和针对那些具有高风险辅助治疗临床试验的患者非常重要。
验证用于预测临床局限性透明细胞 RCC 患者 5 年无复发生存率(RFP)的术后列线图。
设计、设置和参与者:我们从 1990 年至 2009 年在纪念斯隆-凯特琳癌症中心(Memorial Sloan Kettering Cancer Center)确定了所有接受肾切除术治疗的临床局限性透明细胞 RCC 患者。由于数量有限,排除双侧肾肿块、家族性 RCC 综合征和 T3c 或 T4 肿瘤的患者后,共有 1642 名患者可用于分析。
部分或根治性肾切除术。
疾病复发定义为肾切除术后的任何新肿瘤或肾癌特异性死亡率,以先发生者为准。术后列线图用于计算预测的 5 年 RFP,这些值与实际的 5 年 RFP 进行比较。通过一致性指数和校准图评估列线图的性能。
中位随访时间为 39 个月(四分位距:14-79 个月),50 例患者出现疾病复发。列线图的一致性指数为 0.81。校准曲线显示,列线图低估了实际的 5 年 RFP。我们通过纳入整个患者群体更新了列线图,这保持了性能并显著改善了校准。
更新后的透明细胞 RCC 术后列线图在联合队列中表现良好。原始列线图对实际 5 年 RFP 的低估可能是由于外科医生经验的增加和其他未知变量。
我们更新了一种用于评估肾切除术治疗透明细胞肾细胞癌后疾病复发概率的有价值的预测工具。