Yellapa Vijayashree, Devadasan Narayanan, Krumeich Anja, Pant Pai Nitika, Vadnais Caroline, Pai Madhukar, Engel Nora
a Institute of Public Health , Bangalore , India.
b Department of Health, Ethics & Society, Research School for Public Health and Primary Care , Maastricht University , Maastricht , The Netherlands.
Glob Health Action. 2017;10(1):1350452. doi: 10.1080/16549716.2017.1350452.
Depending on a country's diagnostic infrastructure, patients and providers play different roles in ensuring that correct and timely diagnosis is made. However, little is known about the work done by patients in accessing diagnostic services and completing the 'test and treat' loop.
To address this knowledge gap, we traced the diagnostic journeys of patients with tuberculosis, diabetes, hypertension and typhoid, and examined the work they had to do to arrive at a diagnosis.
This paper draws on a qualitative study, which included 78 semi-structured interviews and 13 focus group discussions with patients, public and private healthcare providers, community health workers, test manufacturers, laboratory technicians, program managers and policymakers. Data were collected between January and June 2013 in rural and urban Karnataka, South India, as part of a larger project on barriers to point-of-care testing. We reconstructed patient diagnostic processes retrospectively and analyzed emerging themes and patterns.
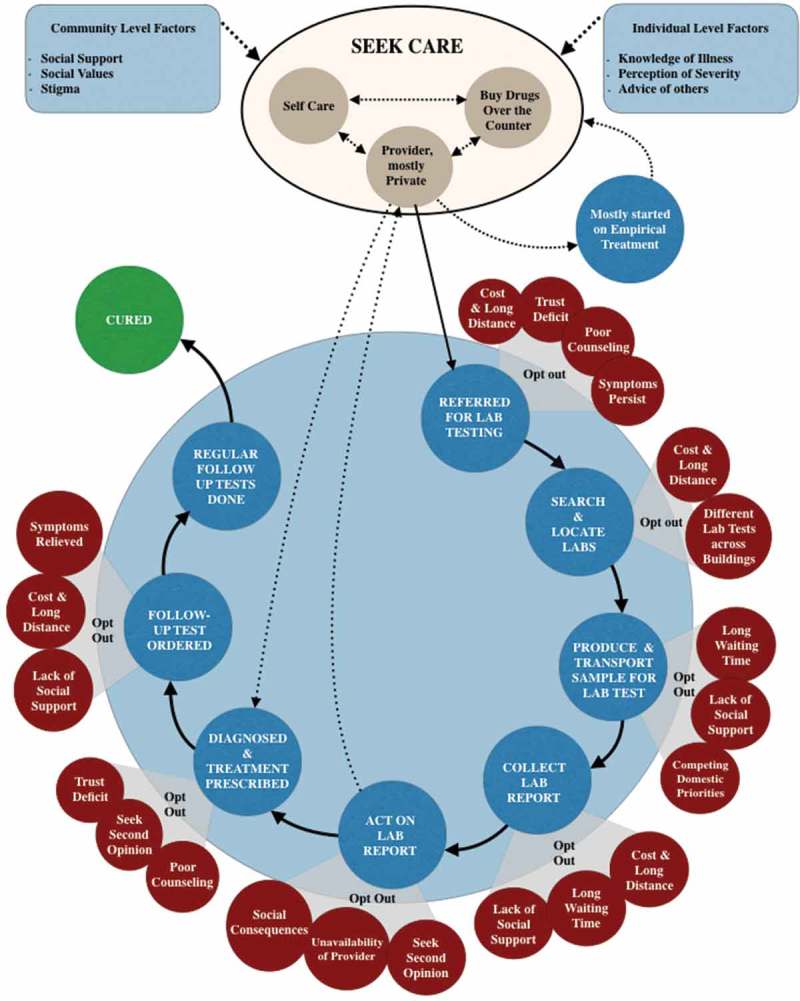
The journey to access diagnostic services requires a high level of involvement and immense work from patients and/or their caretakers. This process entails overcoming cost and distance, negotiating social relations, continuously making sense of their illness and diagnosis, producing and transporting samples, dealing with the social consequences of diagnosis, and returning results to the treating provider. The quality and content of interactions with providers were crucial for completion of test and treat loops. If the tasks became overwhelming, patients opted out, delayed being tested, switched providers and/or reverted to self-testing or self-treatment practices.
Our study demonstrated how difficult it can be for patients to complete diagnostic journeys and how the health system works as far as diagnostics are concerned. If new point-of-care tests are to be implemented successfully, policymakers, program officers and test developers need to find ways to ease patient navigation through diagnostic services.
根据一个国家的诊断基础设施,患者和医疗服务提供者在确保正确及时诊断方面发挥着不同作用。然而,对于患者在获取诊断服务及完成“检测与治疗”循环过程中所做的工作,我们了解甚少。
为填补这一知识空白,我们追踪了结核病、糖尿病、高血压和伤寒患者的诊断过程,并考察了他们为获得诊断所必须做的工作。
本文基于一项定性研究,该研究包括对患者、公立和私立医疗服务提供者、社区卫生工作者、检测产品制造商、实验室技术人员、项目管理人员及政策制定者进行的78次半结构化访谈和13次焦点小组讨论。作为一项关于即时检测障碍的大型项目的一部分,于2013年1月至6月在印度南部卡纳塔克邦的农村和城市地区收集数据。我们回顾性地重构了患者的诊断过程,并分析了新出现的主题和模式。
获取诊断服务的过程需要患者和/或其照料者高度参与并付出大量努力。这一过程需要克服成本和距离问题、协调社会关系、不断理解自身病情和诊断结果、采集和运送样本、应对诊断带来的社会影响以及将检测结果反馈给治疗医生。与医疗服务提供者互动的质量和内容对于完成检测与治疗循环至关重要。如果任务过于繁重,患者会选择放弃、推迟检测、更换医疗服务提供者和/或恢复自我检测或自我治疗。
我们的研究表明患者完成诊断过程可能会多么困难,以及就诊断而言卫生系统是如何运作的。如果要成功实施新的即时检测,政策制定者、项目官员和检测开发者需要找到方法,使患者更轻松地完成诊断服务流程。