Yukich Joshua, Bennett Adam, Yukich Rudy, Stuck Logan, Hamainza Busiku, Silumbe Kafula, Smith Tom, Chitnis Nakul, Steketee Richard W, Finn Timothy, Eisele Thomas P, Miller John M
Center for Applied Malaria Research and Evaluation (CAMRE), Tulane University School of Public Health and Tropical Medicine, New Orleans, LA, 70112, United States.
Global Health Group, University of California San Francisco, San Francisco, CA, United States.
Malar J. 2017 Aug 7;16(1):317. doi: 10.1186/s12936-017-1962-1.
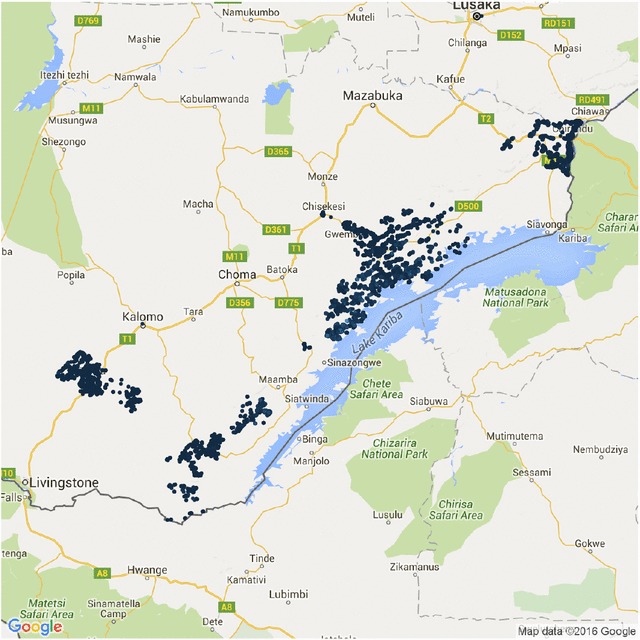
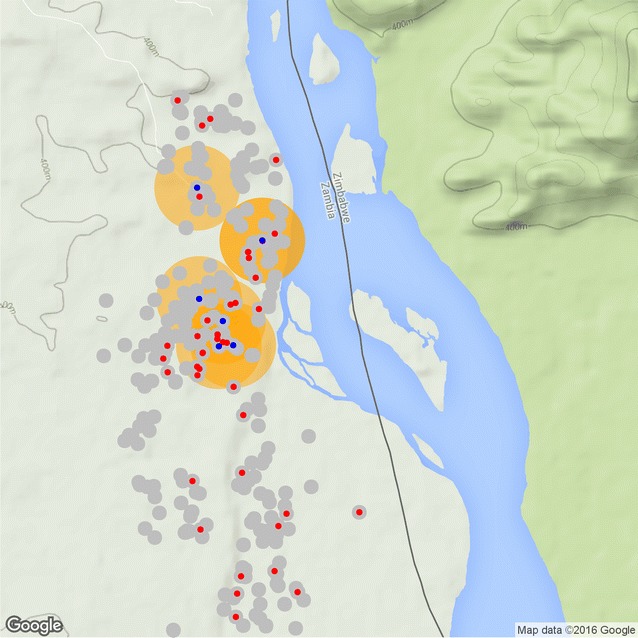
In areas where malaria transmission has been suppressed by vector control interventions many malaria control and elimination programmes are actively seeking new interventions to further reduce malaria prevalence, incidence and transmission. Malaria infection prevalence and incidence has been shown to cluster geographically, especially at lower transmission levels, and as such a reactive strategy is frequently used, by which index cases presenting to a passive surveillance system are used to target small areas for testing and treatment, reactive case detection (RCD), or focal drug administration (fDA). This study utilizes geo-located data from a census with parasitological testing with rapid diagnostic tests (RDTs) and treatment-seeking data collection conducted in southern Zambia to estimate the coverage of RCD or fDA in terms of the population and parasite reservoir as well as the operational requirements of such strategies, using a re-sampling algorithm developed exclusively for this purpose. This re-sampling algorithm allows for the specification of several parameters, such that different operational variants of these reactive strategies can be examined, including varying the search radius, screening for fever, or presumptive treatment (fDA).
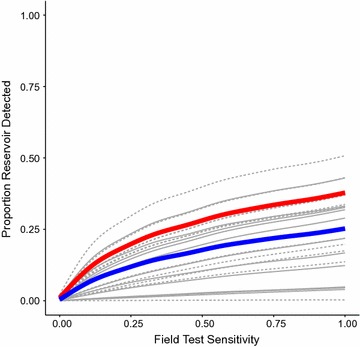
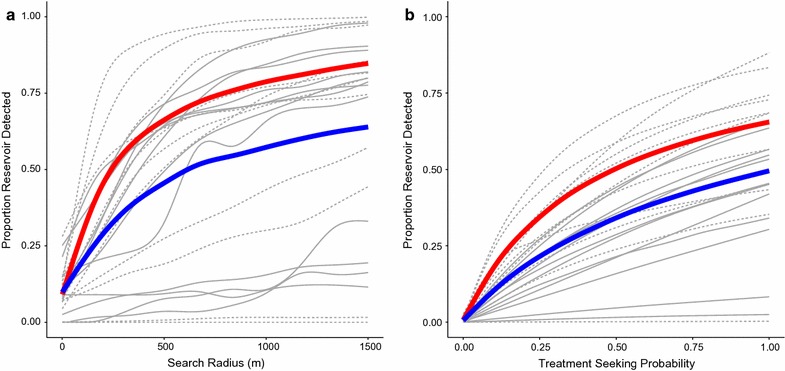
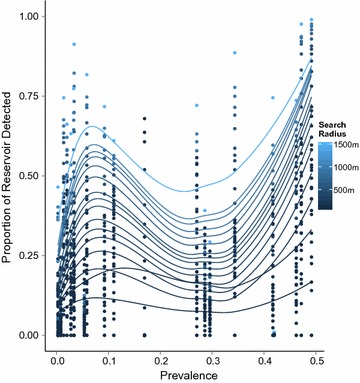
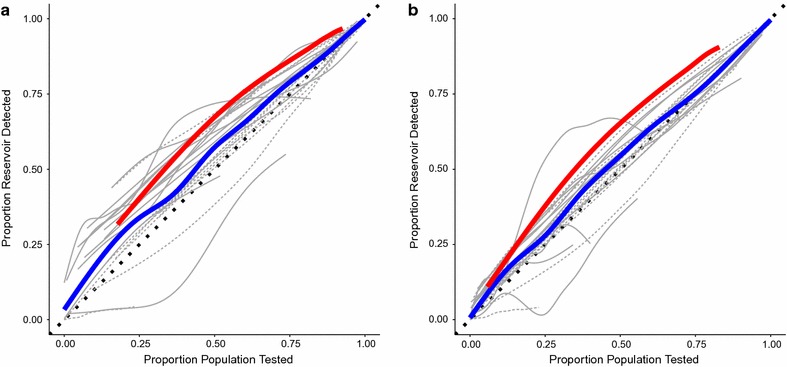
Results indicate that RCD, fDA and active fever screening followed by RCD, even with search radii over several hundered meters will only yield limited coverage of the RDT positive parasite reservoir during a short period. Long-term use of these strategies may increase this proportion. Reactive strategies detect a higher proportion of the reservoir of infections than random searches, but this effect appears to be greater in areas of low, but not moderate malaria prevalence in southern Zambia.
Increases in the sensitivity of RDTs could also affect these results. The number of individuals and households that need to be searched increase rapidly, but approximately linearly with search radius.
Reactive strategies in southern Zambia yield improved identification of the parasite reservoir when targeted to areas with prevalence less than 10%. The operational requirements of delivering reactive strategies routinely are likely to prevent their uptake until prevalence falls far below this level.
在通过病媒控制干预措施抑制了疟疾传播的地区,许多疟疾控制和消除计划正在积极寻求新的干预措施,以进一步降低疟疾流行率、发病率和传播率。疟疾感染流行率和发病率已显示出在地理上呈聚集性,尤其是在较低传播水平时,因此经常采用一种反应性策略,即利用被动监测系统中出现的指示病例来针对小区域进行检测和治疗、反应性病例检测(RCD)或局部药物给药(fDA)。本研究利用赞比亚南部人口普查中的地理位置数据、快速诊断检测(RDT)的寄生虫学检测以及寻求治疗数据收集,使用专门为此目的开发的重采样算法,从人群和寄生虫库的角度估计RCD或fDA的覆盖率以及此类策略的操作要求。这种重采样算法允许指定几个参数,从而可以检查这些反应性策略的不同操作变体,包括改变搜索半径、筛查发热或推定治疗(fDA)。
结果表明,即使搜索半径超过几百米,RCD、fDA以及先进行主动发热筛查再进行RCD,在短时间内对RDT阳性寄生虫库的覆盖率也将有限。长期使用这些策略可能会提高这一比例。反应性策略比随机搜索检测到的感染库比例更高,但在赞比亚南部疟疾流行率低而非中等的地区,这种效果似乎更大。
RDT敏感性的提高也可能影响这些结果。需要搜索的个人和家庭数量迅速增加,但大致与搜索半径呈线性关系。
在赞比亚南部,当针对流行率低于10%的地区时,反应性策略能更好地识别寄生虫库。常规实施反应性策略的操作要求可能会阻碍其采用,直到流行率远低于这一水平。